User login
Dermatologic Care for Refugees: Effective Management of Scabies and Pediculosis
Approximately 108 million individuals have been forcibly displaced across the globe as of 2022, 35 million of whom are formally designated as refugees.1,2 The United States has coordinated resettlement of more refugee populations than any other country; the most common countries of origin are the Democratic Republic of the Congo, Syria, Afghanistan, and Myanmar.3 In 2021, policy to increase the number of refugees resettled in the United States by more than 700% (from 15,000 up to 125,000) was established; since enactment, the United States has seen more than double the refugee arrivals in 2023 than the prior year, making medical care for this population increasingly relevant for the dermatologist.4
Understanding how to care for this population begins with an accurate understanding of the term refugee. The United Nations defines a refugee as a person who is unwilling or unable to return to their country of nationality because of persecution or well-founded fear of persecution due to race, religion, nationality, membership in a particular social group, or political opinion. This term grants a protected status under international law and encompasses access to travel assistance, housing, cultural orientation, and medical evaluation upon resettlement.5,6
The burden of treatable dermatologic conditions in refugee populations ranges from 19% to 96% in the literature7,8 and varies from inflammatory disorders to infectious and parasitic diseases.9 In one study of 6899 displaced individuals in Greece, the prevalence of dermatologic conditions was higher than traumatic injury, cardiac disease, psychological conditions, and dental disease.10
When outlining differential diagnoses for parasitic infestations of the skin that affect refugee populations, helpful considerations include the individual’s country of origin, route traveled, and method of travel.11 Parasitic infestations specifically are more common in refugee populations when there are barriers to basic hygiene, crowded living or travel conditions, or lack of access to health care, which they may experience at any point in their home country, during travel, or in resettlement housing.8
Even with limited examination and diagnostic resources, the skin is the most accessible first indication of patients’ overall well-being and often provides simple diagnostic clues—in combination with contextualization of the patient’s unique circumstances—necessary for successful diagnosis and treatment of scabies and pediculosis.12 The dermatologist working with refugee populations may be the first set of eyes available and trained to discern skin infestations and therefore has the potential to improve overall outcomes.
Some parasitic infestations in refugee populations may fall under the category of neglected tropical diseases, including scabies, ascariasis, trypanosomiasis, leishmaniasis, and schistosomiasis; they affect an estimated 1 billion individuals across the globe but historically have been underrepresented in the literature and in health policy due in part to limited access to care.13 This review will focus on infestations by the scabies mite (Sarcoptes scabiei var hominis) and the human louse, as these frequently are encountered, easily diagnosed, and treatable by trained clinicians, even in resource-limited settings.
Scabies
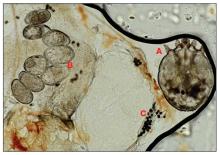
Scabies is a parasitic skin infestation caused by the 8-legged mite Sarcoptes scabiei var hominis. The female mite begins the infestation process via penetration of the epidermis, particularly the stratum corneum, and commences laying eggs (Figure 1). The subsequent larvae emerge 48 to 72 hours later and remain burrowed in the epidermis. The larvae mature over the next 10 to 14 days and continue the reproductive cycle.14,15 Symptoms of infestation occurs due to a hypersensitivity reaction to the mite and its by-products.16 Transmission of the mite primarily occurs via direct (skin-to-skin) contact with infected individuals or environmental surfaces for 24 to36 hours in specific conditions, though the latter source has been debated in the literature.
The method of transmission is particularly important when considering care for refugee populations. Scabies is found most often in those living in or traveling from tropical regions including East Asia, Southeast Asia, Oceania, and Latin America.17 In displaced or refugee populations, a lack of access to basic hygiene, extended travel in close quarters, and suboptimal health care access all may lead to an increased incidence of untreated scabies infestations.18 Scabies is more prevalent in children, with increased potential for secondary bacterial infections with Streptococcus and Staphylococcus species due to excoriation in unsanitary conditions. Secondary infection with Streptococcus pyogenes can lead to acute poststreptococcal glomerulonephritis, which accounts for a large burden of chronic kidney disease in affected populations.19 However, scabies may be found in any population, regardless of hygiene or health care access. Treating health care providers should keep a broad differential.
Presentation—The latency of scabies symptoms is 2 to 6 weeks in a primary outbreak and may be as short as 1 to 3 days with re-infestation, following the course of delayed-type hypersensitivity.20 The initial hallmark symptom is pruritus with increased severity in the evening. Visible lesions, excoriations, and burrows associated with scattered vesicles or pustules may be seen over the web spaces of the hands and feet, volar surfaces of the wrists, axillae, waist, genitalia, inner thighs, or buttocks.19 Chronic infestation often manifests with genital nodules. In populations with limited access to health care, there are reports of a sensitization phenomenon in which the individual may become less symptomatic after 4 to 6 weeks and yet be a potential carrier of the mite.21
Those with compromised immune function, such as individuals living with HIV or severe malnutrition, may present with crusted scabies, a variant that manifests as widespread hyperkeratotic scaling with more pronounced involvement of the head, neck, and acral areas. In contrast to classic scabies, crusted scabies is associated with minimal pruritus.22
Diagnosis—The diagnosis of scabies is largely clinical with confirmation through skin scrapings. The International Alliance for Control of Scabies has established diagnostic criteria that include a combination of clinical findings, history, and visualization of mites.23 A dermatologist working with refugee populations may employ any combination of history (eg, nocturnal itch, exposure to an affected individual) or clinical findings along with a high degree of suspicion in those with elevated risk. Visualization of mites is helpful to confirm the diagnosis and may be completed with the application of mineral oil at the terminal end of a burrow, skin scraping with a surgical blade or needle, and examination under light microscopy.
Treatment—First-line treatment for scabies consists of application of permethrin cream 5% on the skin of the neck to the soles of the feet, which is to be left on for 8 to 14 hours followed by rinsing. Re-application is recommended in 1 to 2 weeks. Oral ivermectin is a reasonable alternative to permethrin cream due to its low cost and easy administration in large affected groups. It is not labeled for use in pregnant women or children weighing less than 15 kg but has no selective fetal toxicity. Treatment of scabies with ivermectin has the benefit of treating many other parasitic infections. Both medications are on the World Health Organization Model List of Essential Medications and are widely available for treating providers, even in resource-limited settings.24
Much of the world still uses benzyl benzoate or precipitated sulfur ointment to treat scabies, and some botanicals used in folk medicine have genuine antiscabetic properties. Pruritus may persist for 1 to 4 weeks following treatment and does not indicate treatment failure. Topical camphor and menthol preparations, low-potency topical corticosteroids, or emollients all may be employed for relief.25Sarna is a Spanish term for scabies and has become the proprietary name for topical antipruritic agents. Additional methods of treatment and prevention include washing clothes and linens in hot water and drying on high heat. If machine washing is not available, clothing and linens may be sealed in a plastic bag for 72 hours.
Pediculosis
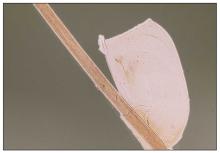
Pediculosis is an infestation caused by the ectoparasite Pediculus humanus, an obligate, sesame seed–sized louse that feeds exclusively on the blood of its host (Figure 2).26 Of the lice species, 2 require humans as hosts; one is P humanus and the other is Pthirus pubis (pubic lice). Pediculus humanus may be further classified into morphologies based largely on the affected area: body (P humanus corporis) or head (P humanus capitis), both of which will be discussed.27

Lice primarily attach to clothing and hair shafts, then transfer to the skin for blood feeds. Females lay eggs that hatch 6 to 10 days later, subsequently maturing into adults. The lifespan of these parasites with regular access to a host is 1 to 3 months for head lice and 18 days for body lice vs only 3 to 5 days without a host.28 Transmission of P humanus capitis primarily occurs via direct contact with affected individuals, either head-to-head contact or sharing of items such as brushes and headscarves; P humanus corporis also may be transmitted via direct contact with affected individuals or clothing.
Pediculosis is an important infestation to consider when providing care for refugee populations. Risk factors include lack of access to basic hygiene, including regular bathing or laundering of clothing, and crowded conditions that make direct person-to-person contact with affected individuals more likely.29 Body lice are associated more often with domestic turbulence and displaced populations30 in comparison to head lice, which have broad demographic variables, most often affecting females and children.28 Fatty acids in adult male sebum make the scalp less hospitable to lice.
Presentation—The most common clinical manifestation of pediculosis is pruritus. Cutaneous findings can include papules, wheals, or hemorrhagic puncta secondary to the louse bite. Due to the Tyndall effect of deep hemosiderin pigment, blue-grey macules termed maculae ceruleae (Figure 3) also may be present in chronic infestations of pediculosis pubis, in contrast to pediculosis capitis or corporis.31 Body louse infestation is associated with a general pruritus concentrated on the neck, shoulders, and waist—areas where clothing makes the most direct contact. Lesions may be visible and include eczematous patches with excoriation and possible secondary bacterial infection. Chronic infestation may exhibit lichenification or hyperpigmentation in associated areas. Head lice most often manifest with localized scalp pruritus and associated excoriation and cervical or occipital lymphadenopathy.32

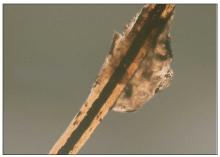
Diagnosis—The diagnosis of pediculosis is clinical, with confirmation requiring direct examination of the insect or nits (the egg case of the parasite)(Figure 4). Body lice and associated nits can be visualized on clothing seams near areas of highest body temperature, particularly the waistband. Head lice may be visualized crawling on hair shafts or on a louse comb. Nits are firmly attached to hair shafts and are visible to the naked eye, whereas pseudonits slide freely along the hair shaft and are not a manifestation of louse infestation (Figure 5).31
Treatment—Treatment varies by affected area. Pediculosis corporis may be treated with permethrin cream 5% applied to the entire body and left on for 8 to 10 hours, but this may not be necessary if facilities are available to wash and dry clothing.33 The use of oral ivermectin and permethrin-impregnated underwear both have been proposed.34,35 Treatment of pediculosis capitis may be accomplished with a variety of topical pediculicides including permethrin, pyrethrum with piperonyl butoxide, dimethicone, malathion, benzyl alcohol, spinosad, and topical ivermectin.22 Topical corticosteroids or emollients may be employed for residual pruritus.
Equally important is environmental elimination of infestation. Clothing should be discarded if possible or washed and dried using high heat. If neither approach is possible or appropriate, clothing may be sealed in a plastic bag for 2 weeks or treated with a pediculicide. Nit combing is an important adjunct in the treatment of pediculosis capitis.36 It is important to encourage return to work and/or school immediately after treatment. “No nit” policies are more harmful to education than helpful for prevention of investation.37
Pediculosis corporis may transmit infectious agents including Bartonella quintana, (trench fever, endocarditis, bacillary angiomatosis), Borrelia recurrentis (louse-borne relapsing fever), and Rickettsia prowazekii (epidemic typhus).31,38,39 Additionally, severe pediculosis infestations have the potential to cause chronic blood loss in affected populations. In a study of patients with active pediculosis infestation, mean hemoglobin values were found to be 2.5 g/dL lower than a matched population without infestation.40 It is important to consider pediculosis as a risk for iron-deficiency anemia in populations who are known to lack access to regular medical evaluation.41
Future Considerations
Increased access to tools and education for clinicians treating refugee populations is key to reducing the burden of parasitic skin disease and related morbidity and mortality in vulnerable groups both domestically and globally. One such tool, the Skin NTDs App, was launched by the World Health Organization in 2020. It is available for free for Android and iOS devices to assist clinicians in the field with the diagnosis and treatment of neglected tropical diseases—including scabies—that may affect refugee populations.42
Additionally, to both improve access and limit preventable sequelae, future investigations into appropriate models of community-based care are paramount. The model of community-based care is centered on the idea of care provision that prioritizes safety, accessibility, affordability, and acceptability in an environment closest to vulnerable populations. The largest dermatologic society, the International League of Dermatological Societies, formed a Migrant Health Dermatology Working Group that prioritizes understanding and improving care for refugee and migrant populations; this group hosted a summit in 2022, bringing together international subject matter leaders to discuss such models of care and set goals for the creation of tool kits for patients, frontline health care workers, and dermatologists.43
Conclusion
Improvement in dermatologic care of refugee populations includes provision of culturally and linguistically appropriate care by trained clinicians, adequate access to the most essential medications, and basic physical or legal access to health care systems in general.8,11,44 Parasitic infestations have the potential to remain asymptomatic for extended periods of time and result in spread to potentially nonendemic regions of resettlement.45 Additionally, the psychosocial well-being of refugee populations upon resettlement may be negatively affected by stigma of disease processes such as scabies and pediculosis, leading to additional barriers to successful re-entry into the patient’s new environment.46 Therefore, proper screening, diagnosis, and treatment of the most common parasitic infestations in this population have great potential to improve outcomes for large groups across the globe.
- Monin K, Batalova J, Lai T. Refugees and Asylees in the United States. Migration Information Source. Published May 13, 2021. Accessed April 4, 2024. https://www.migrationpolicy.org/article/refugees-and-asylees-united-states-2021
- UNHCR. Figures at a Glance. UNHCR USA. Update June 14, 2023. Accessed April 4, 2024. https://www.unhcr.org/en-us/figures-at-a-glance.html
- UNHCR. Refugee resettlement facts. Published October 2023. Accessed April 8, 2024. https://www.unhcr.org/us/media/refugee-resettlement-facts
- US Department of State. Report to Congress on Proposed Refugee Admissions for Fiscal Year 2024. Published November 3, 2023. Accessed April 8, 2024. https://www.state.gov/report-to-congress-on-proposed-refugee-admissions-for-fiscal-year-2024/
- UNHCR. Compact for Migration: Definitions. United Nations. Accessed April 4, 2024. https://refugeesmigrants.un.org/definitions
- United Nations High Commissioner for Refugees (UNHCR). Convention and Protocol Relating to the Status of Refugees. Published December 2010. Accessed January 11, 2024. https://www.unhcr.org/us/media/convention-and-protocol-relating-status-refugees
- Kibar Öztürk M. Skin diseases in rural Nyala, Sudan (in a rural hospital, in 12 orphanages, and in two refugee camps). Int J Dermatol. 2019;58:1341-1349. doi:10.1111/ijd.14619
- Padovese V, Knapp A. Challenges of managing skin diseases in refugees and migrants. Dermatol Clin. 2021;39:101-115. doi:10.1016/j.det.2020.08.010
- Saikal SL, Ge L, Mir A, et al. Skin disease profile of Syrian refugees in Jordan: a field-mission assessment. J Eur Acad Dermatol Venereol. 2020;34:419-425. doi:10.1111/jdv.15909
- Eonomopoulou A, Pavli A, Stasinopoulou P, et al. Migrant screening: lessons learned from the migrant holding level at the Greek-Turkish borders. J Infect Public Health. 2017;10:177-184. doi:10.1016/j.jiph.2016.04.012
- Marano N, Angelo KM, Merrill RD, et al. Expanding travel medicine in the 21st century to address the health needs of the world’s migrants.J Travel Med. 2018;25. doi:10.1093/jtm/tay067
- Hay RJ, Asiedu K. Skin-related neglected tropical diseases (skin NTDs)—a new challenge. Trop Med Infect Dis. 2018;4. doi:10.3390/tropicalmed4010004
- NIAID. Neglected tropical diseases. Updated July 11, 2016. Accessed April 4, 2024. https://www.niaid.nih.gov/research/neglected-tropical-diseases
- Arlian LG, Morgan MS. A review of Sarcoptes scabiei: past, present and future. Parasit Vectors. 2017;10:297. doi:10.1186/s13071-017-2234-1
- Arlian LG, Runyan RA, Achar S, et al. Survival and infectivity of Sarcoptes scabiei var. canis and var. hominis. J Am Acad Dermatol. 1984;11(2 pt 1):210-215. doi:10.1016/s0190-9622(84)70151-4
- Chandler DJ, Fuller LC. A review of scabies: an infestation more than skin deep. Dermatology. 2019;235:79-90. doi:10.1159/000495290
- Karimkhani C, Colombara DV, Drucker AM, et al. The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17:1247-1254. doi:10.1016/S1473-3099(17)30483-8
- Romani L, Steer AC, Whitfeld MJ, et al. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet Infect Dis. 2015;15:960-967. doi:10.1016/S1473-3099(15)00132-2
- Thomas C, Coates SJ, Engelman D, et al. Ectoparasites: scabies. J Am Acad Dermatol. 2020;82:533-548. doi:10.1016/j.jaad.2019.05.109
- Mellanby K, Johnson CG, Bartley WC. Treatment of scabies. Br Med J. 1942;2:1-4. doi:10.1136/bmj.2.4252.1
- Walton SF. The immunology of susceptibility and resistance to scabies. Parasit Immunol. 2010;32:532-540. doi:10.1111/j.1365-3024.2010.01218.x
- Coates SJ, Thomas C, Chosidow O, et al. Ectoparasites: pediculosis and tungiasis. J Am Acad Dermatol. 2020;82:551-569. doi:10.1016/j.jaad.2019.05.110
- Engelman D, Fuller LC, Steer AC; International Alliance for the Control of Scabies Delphi p. Consensus criteria for the diagnosis of scabies: a Delphi study of international experts. PLoS Negl Trop Dis. 2018;12:E0006549. doi:10.1371/journal.pntd.0006549
- World Health Organization. WHO Model Lists of Essential Medicines—23rd list, 2023. Updated July 26, 2023. Accessed April 8, 2024. https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Badiaga S, Brouqui P. Human louse-transmitted infectious diseases. Clin Microbiol Infect. 2012;18:332-337. doi:10.1111/j.1469-0691.2012.03778.x
- Leo NP, Campbell NJH, Yang X, et al. Evidence from mitochondrial DNA that head lice and body lice of humans (Phthiraptera: Pediculidae) are conspecific. J Med Entomol. 2002;39:662-666. doi:10.1603/0022-2585-39.4.662
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826. doi:10.1016/S0140-6736(99)09458-1
- Arnaud A, Chosidow O, Détrez M-A, et al. Prevalences of scabies and pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112. doi:10.1111/bjd.14226
- Brouqui P. Arthropod-borne diseases associated with political and social disorder. Annu Rev Entomol. 2011;56:357-374. doi:10.1146/annurev-ento-120709-144739
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12. doi:10.1016/S0190-9622(03)02729-4
- Bloomfield D. Head lice. Pediatr Rev. 2002;23:34-35; discussion 34-35. doi:10.1542/pir.23-1-34
- Stone SP GJ, Bacelieri RE. Scabies, other mites, and pediculosis. In: Wolf K GL, Katz SI, et al (eds). Fitzpatrick’s Dermatology in General Medicine. McGraw Hill; 2008:2029.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476. doi:10.1086/499279
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279. doi:10.1001/jamadermatol.2013.6398
- CDC. Parasites: Treatment. Updated October 15, 2019. Accessed April 4, 2024. https://www.cdc.gov/parasites/lice/head/treatment.html
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:e1355-e1365. doi:10.1542/peds.2015-0746
- Ohl ME, Spach DH. Bartonella quintana and urban trench fever. Clin Infect Dis. 2000;31:131-135. doi:10.1086/313890
- Drali R, Sangaré AK, Boutellis A, et al. Bartonella quintana in body lice from scalp hair of homeless persons, France. Emerg Infect Dis. 2014;20:907-908. doi:10.3201/eid2005.131242
- Rudd N, Zakaria A, Kohn MA, et al. Association of body lice infestation with hemoglobin values in hospitalized dermatology patients. JAMA Dermatol. 2022;158:691-693. doi:10.1001/jamadermatol.2022.0818
- Guss DA, Koenig M, Castillo EM. Severe iron deficiency anemia and lice infestation. J Emergency Med. 2011;41:362-365. doi:10.1016/j.jemermed.2010.05.030
- Neglected tropical diseases of the skin: WHO launches mobile application to facilitate diagnosis. News release. World Health Organization; July 16, 2020. Accessed April 4, 2024. https://www.who.int/news/item/16-07-2020-neglected-tropical-diseases-of-the-skin-who-launches-mobile-application-to-facilitate-diagnosis
- Padovese V, Fuller LC, Griffiths CEM, et al; Migrant Health Dermatology Working Group of the International Foundation for Dermatology. Migrant skin health: perspectives from the Migrant Health Summit, Malta, 2022. Br J Dermatology. 2023;188:553-554. doi:10.1093/bjd/ljad001
- Knapp AP, Rehmus W, Chang AY. Skin diseases in displaced populations: a review of contributing factors, challenges, and approaches to care. Int J Dermatol. 2020;59:1299-1311. doi:10.1111/ijd.15063
- Norman FF, Comeche B, Chamorro S, et al. Overcoming challenges in the diagnosis and treatment of parasitic infectious diseases in migrants. Expert Rev Anti-infective Therapy. 2020;18:127-143. doi:10.1080/14787210.2020.1713099
- Skin NTDs: prioritizing integrated approaches to reduce suffering, psychosocial impact and stigmatization. News release. World Health Organization; October 29, 2020. Accessed April 4, 2024. https://www.who.int/news/item/29-10-2020-skin-ntds-prioritizing-integrated-approaches-to-reduce-suffering-psychosocial-impact-and-stigmatization
Approximately 108 million individuals have been forcibly displaced across the globe as of 2022, 35 million of whom are formally designated as refugees.1,2 The United States has coordinated resettlement of more refugee populations than any other country; the most common countries of origin are the Democratic Republic of the Congo, Syria, Afghanistan, and Myanmar.3 In 2021, policy to increase the number of refugees resettled in the United States by more than 700% (from 15,000 up to 125,000) was established; since enactment, the United States has seen more than double the refugee arrivals in 2023 than the prior year, making medical care for this population increasingly relevant for the dermatologist.4
Understanding how to care for this population begins with an accurate understanding of the term refugee. The United Nations defines a refugee as a person who is unwilling or unable to return to their country of nationality because of persecution or well-founded fear of persecution due to race, religion, nationality, membership in a particular social group, or political opinion. This term grants a protected status under international law and encompasses access to travel assistance, housing, cultural orientation, and medical evaluation upon resettlement.5,6
The burden of treatable dermatologic conditions in refugee populations ranges from 19% to 96% in the literature7,8 and varies from inflammatory disorders to infectious and parasitic diseases.9 In one study of 6899 displaced individuals in Greece, the prevalence of dermatologic conditions was higher than traumatic injury, cardiac disease, psychological conditions, and dental disease.10
When outlining differential diagnoses for parasitic infestations of the skin that affect refugee populations, helpful considerations include the individual’s country of origin, route traveled, and method of travel.11 Parasitic infestations specifically are more common in refugee populations when there are barriers to basic hygiene, crowded living or travel conditions, or lack of access to health care, which they may experience at any point in their home country, during travel, or in resettlement housing.8
Even with limited examination and diagnostic resources, the skin is the most accessible first indication of patients’ overall well-being and often provides simple diagnostic clues—in combination with contextualization of the patient’s unique circumstances—necessary for successful diagnosis and treatment of scabies and pediculosis.12 The dermatologist working with refugee populations may be the first set of eyes available and trained to discern skin infestations and therefore has the potential to improve overall outcomes.
Some parasitic infestations in refugee populations may fall under the category of neglected tropical diseases, including scabies, ascariasis, trypanosomiasis, leishmaniasis, and schistosomiasis; they affect an estimated 1 billion individuals across the globe but historically have been underrepresented in the literature and in health policy due in part to limited access to care.13 This review will focus on infestations by the scabies mite (Sarcoptes scabiei var hominis) and the human louse, as these frequently are encountered, easily diagnosed, and treatable by trained clinicians, even in resource-limited settings.
Scabies
Scabies is a parasitic skin infestation caused by the 8-legged mite Sarcoptes scabiei var hominis. The female mite begins the infestation process via penetration of the epidermis, particularly the stratum corneum, and commences laying eggs (Figure 1). The subsequent larvae emerge 48 to 72 hours later and remain burrowed in the epidermis. The larvae mature over the next 10 to 14 days and continue the reproductive cycle.14,15 Symptoms of infestation occurs due to a hypersensitivity reaction to the mite and its by-products.16 Transmission of the mite primarily occurs via direct (skin-to-skin) contact with infected individuals or environmental surfaces for 24 to36 hours in specific conditions, though the latter source has been debated in the literature.
The method of transmission is particularly important when considering care for refugee populations. Scabies is found most often in those living in or traveling from tropical regions including East Asia, Southeast Asia, Oceania, and Latin America.17 In displaced or refugee populations, a lack of access to basic hygiene, extended travel in close quarters, and suboptimal health care access all may lead to an increased incidence of untreated scabies infestations.18 Scabies is more prevalent in children, with increased potential for secondary bacterial infections with Streptococcus and Staphylococcus species due to excoriation in unsanitary conditions. Secondary infection with Streptococcus pyogenes can lead to acute poststreptococcal glomerulonephritis, which accounts for a large burden of chronic kidney disease in affected populations.19 However, scabies may be found in any population, regardless of hygiene or health care access. Treating health care providers should keep a broad differential.
Presentation—The latency of scabies symptoms is 2 to 6 weeks in a primary outbreak and may be as short as 1 to 3 days with re-infestation, following the course of delayed-type hypersensitivity.20 The initial hallmark symptom is pruritus with increased severity in the evening. Visible lesions, excoriations, and burrows associated with scattered vesicles or pustules may be seen over the web spaces of the hands and feet, volar surfaces of the wrists, axillae, waist, genitalia, inner thighs, or buttocks.19 Chronic infestation often manifests with genital nodules. In populations with limited access to health care, there are reports of a sensitization phenomenon in which the individual may become less symptomatic after 4 to 6 weeks and yet be a potential carrier of the mite.21
Those with compromised immune function, such as individuals living with HIV or severe malnutrition, may present with crusted scabies, a variant that manifests as widespread hyperkeratotic scaling with more pronounced involvement of the head, neck, and acral areas. In contrast to classic scabies, crusted scabies is associated with minimal pruritus.22
Diagnosis—The diagnosis of scabies is largely clinical with confirmation through skin scrapings. The International Alliance for Control of Scabies has established diagnostic criteria that include a combination of clinical findings, history, and visualization of mites.23 A dermatologist working with refugee populations may employ any combination of history (eg, nocturnal itch, exposure to an affected individual) or clinical findings along with a high degree of suspicion in those with elevated risk. Visualization of mites is helpful to confirm the diagnosis and may be completed with the application of mineral oil at the terminal end of a burrow, skin scraping with a surgical blade or needle, and examination under light microscopy.
Treatment—First-line treatment for scabies consists of application of permethrin cream 5% on the skin of the neck to the soles of the feet, which is to be left on for 8 to 14 hours followed by rinsing. Re-application is recommended in 1 to 2 weeks. Oral ivermectin is a reasonable alternative to permethrin cream due to its low cost and easy administration in large affected groups. It is not labeled for use in pregnant women or children weighing less than 15 kg but has no selective fetal toxicity. Treatment of scabies with ivermectin has the benefit of treating many other parasitic infections. Both medications are on the World Health Organization Model List of Essential Medications and are widely available for treating providers, even in resource-limited settings.24
Much of the world still uses benzyl benzoate or precipitated sulfur ointment to treat scabies, and some botanicals used in folk medicine have genuine antiscabetic properties. Pruritus may persist for 1 to 4 weeks following treatment and does not indicate treatment failure. Topical camphor and menthol preparations, low-potency topical corticosteroids, or emollients all may be employed for relief.25Sarna is a Spanish term for scabies and has become the proprietary name for topical antipruritic agents. Additional methods of treatment and prevention include washing clothes and linens in hot water and drying on high heat. If machine washing is not available, clothing and linens may be sealed in a plastic bag for 72 hours.
Pediculosis
Pediculosis is an infestation caused by the ectoparasite Pediculus humanus, an obligate, sesame seed–sized louse that feeds exclusively on the blood of its host (Figure 2).26 Of the lice species, 2 require humans as hosts; one is P humanus and the other is Pthirus pubis (pubic lice). Pediculus humanus may be further classified into morphologies based largely on the affected area: body (P humanus corporis) or head (P humanus capitis), both of which will be discussed.27
Lice primarily attach to clothing and hair shafts, then transfer to the skin for blood feeds. Females lay eggs that hatch 6 to 10 days later, subsequently maturing into adults. The lifespan of these parasites with regular access to a host is 1 to 3 months for head lice and 18 days for body lice vs only 3 to 5 days without a host.28 Transmission of P humanus capitis primarily occurs via direct contact with affected individuals, either head-to-head contact or sharing of items such as brushes and headscarves; P humanus corporis also may be transmitted via direct contact with affected individuals or clothing.
Pediculosis is an important infestation to consider when providing care for refugee populations. Risk factors include lack of access to basic hygiene, including regular bathing or laundering of clothing, and crowded conditions that make direct person-to-person contact with affected individuals more likely.29 Body lice are associated more often with domestic turbulence and displaced populations30 in comparison to head lice, which have broad demographic variables, most often affecting females and children.28 Fatty acids in adult male sebum make the scalp less hospitable to lice.
Presentation—The most common clinical manifestation of pediculosis is pruritus. Cutaneous findings can include papules, wheals, or hemorrhagic puncta secondary to the louse bite. Due to the Tyndall effect of deep hemosiderin pigment, blue-grey macules termed maculae ceruleae (Figure 3) also may be present in chronic infestations of pediculosis pubis, in contrast to pediculosis capitis or corporis.31 Body louse infestation is associated with a general pruritus concentrated on the neck, shoulders, and waist—areas where clothing makes the most direct contact. Lesions may be visible and include eczematous patches with excoriation and possible secondary bacterial infection. Chronic infestation may exhibit lichenification or hyperpigmentation in associated areas. Head lice most often manifest with localized scalp pruritus and associated excoriation and cervical or occipital lymphadenopathy.32
Diagnosis—The diagnosis of pediculosis is clinical, with confirmation requiring direct examination of the insect or nits (the egg case of the parasite)(Figure 4). Body lice and associated nits can be visualized on clothing seams near areas of highest body temperature, particularly the waistband. Head lice may be visualized crawling on hair shafts or on a louse comb. Nits are firmly attached to hair shafts and are visible to the naked eye, whereas pseudonits slide freely along the hair shaft and are not a manifestation of louse infestation (Figure 5).31
Treatment—Treatment varies by affected area. Pediculosis corporis may be treated with permethrin cream 5% applied to the entire body and left on for 8 to 10 hours, but this may not be necessary if facilities are available to wash and dry clothing.33 The use of oral ivermectin and permethrin-impregnated underwear both have been proposed.34,35 Treatment of pediculosis capitis may be accomplished with a variety of topical pediculicides including permethrin, pyrethrum with piperonyl butoxide, dimethicone, malathion, benzyl alcohol, spinosad, and topical ivermectin.22 Topical corticosteroids or emollients may be employed for residual pruritus.
Equally important is environmental elimination of infestation. Clothing should be discarded if possible or washed and dried using high heat. If neither approach is possible or appropriate, clothing may be sealed in a plastic bag for 2 weeks or treated with a pediculicide. Nit combing is an important adjunct in the treatment of pediculosis capitis.36 It is important to encourage return to work and/or school immediately after treatment. “No nit” policies are more harmful to education than helpful for prevention of investation.37
Pediculosis corporis may transmit infectious agents including Bartonella quintana, (trench fever, endocarditis, bacillary angiomatosis), Borrelia recurrentis (louse-borne relapsing fever), and Rickettsia prowazekii (epidemic typhus).31,38,39 Additionally, severe pediculosis infestations have the potential to cause chronic blood loss in affected populations. In a study of patients with active pediculosis infestation, mean hemoglobin values were found to be 2.5 g/dL lower than a matched population without infestation.40 It is important to consider pediculosis as a risk for iron-deficiency anemia in populations who are known to lack access to regular medical evaluation.41
Future Considerations
Increased access to tools and education for clinicians treating refugee populations is key to reducing the burden of parasitic skin disease and related morbidity and mortality in vulnerable groups both domestically and globally. One such tool, the Skin NTDs App, was launched by the World Health Organization in 2020. It is available for free for Android and iOS devices to assist clinicians in the field with the diagnosis and treatment of neglected tropical diseases—including scabies—that may affect refugee populations.42
Additionally, to both improve access and limit preventable sequelae, future investigations into appropriate models of community-based care are paramount. The model of community-based care is centered on the idea of care provision that prioritizes safety, accessibility, affordability, and acceptability in an environment closest to vulnerable populations. The largest dermatologic society, the International League of Dermatological Societies, formed a Migrant Health Dermatology Working Group that prioritizes understanding and improving care for refugee and migrant populations; this group hosted a summit in 2022, bringing together international subject matter leaders to discuss such models of care and set goals for the creation of tool kits for patients, frontline health care workers, and dermatologists.43
Conclusion
Improvement in dermatologic care of refugee populations includes provision of culturally and linguistically appropriate care by trained clinicians, adequate access to the most essential medications, and basic physical or legal access to health care systems in general.8,11,44 Parasitic infestations have the potential to remain asymptomatic for extended periods of time and result in spread to potentially nonendemic regions of resettlement.45 Additionally, the psychosocial well-being of refugee populations upon resettlement may be negatively affected by stigma of disease processes such as scabies and pediculosis, leading to additional barriers to successful re-entry into the patient’s new environment.46 Therefore, proper screening, diagnosis, and treatment of the most common parasitic infestations in this population have great potential to improve outcomes for large groups across the globe.
Approximately 108 million individuals have been forcibly displaced across the globe as of 2022, 35 million of whom are formally designated as refugees.1,2 The United States has coordinated resettlement of more refugee populations than any other country; the most common countries of origin are the Democratic Republic of the Congo, Syria, Afghanistan, and Myanmar.3 In 2021, policy to increase the number of refugees resettled in the United States by more than 700% (from 15,000 up to 125,000) was established; since enactment, the United States has seen more than double the refugee arrivals in 2023 than the prior year, making medical care for this population increasingly relevant for the dermatologist.4
Understanding how to care for this population begins with an accurate understanding of the term refugee. The United Nations defines a refugee as a person who is unwilling or unable to return to their country of nationality because of persecution or well-founded fear of persecution due to race, religion, nationality, membership in a particular social group, or political opinion. This term grants a protected status under international law and encompasses access to travel assistance, housing, cultural orientation, and medical evaluation upon resettlement.5,6
The burden of treatable dermatologic conditions in refugee populations ranges from 19% to 96% in the literature7,8 and varies from inflammatory disorders to infectious and parasitic diseases.9 In one study of 6899 displaced individuals in Greece, the prevalence of dermatologic conditions was higher than traumatic injury, cardiac disease, psychological conditions, and dental disease.10
When outlining differential diagnoses for parasitic infestations of the skin that affect refugee populations, helpful considerations include the individual’s country of origin, route traveled, and method of travel.11 Parasitic infestations specifically are more common in refugee populations when there are barriers to basic hygiene, crowded living or travel conditions, or lack of access to health care, which they may experience at any point in their home country, during travel, or in resettlement housing.8
Even with limited examination and diagnostic resources, the skin is the most accessible first indication of patients’ overall well-being and often provides simple diagnostic clues—in combination with contextualization of the patient’s unique circumstances—necessary for successful diagnosis and treatment of scabies and pediculosis.12 The dermatologist working with refugee populations may be the first set of eyes available and trained to discern skin infestations and therefore has the potential to improve overall outcomes.
Some parasitic infestations in refugee populations may fall under the category of neglected tropical diseases, including scabies, ascariasis, trypanosomiasis, leishmaniasis, and schistosomiasis; they affect an estimated 1 billion individuals across the globe but historically have been underrepresented in the literature and in health policy due in part to limited access to care.13 This review will focus on infestations by the scabies mite (Sarcoptes scabiei var hominis) and the human louse, as these frequently are encountered, easily diagnosed, and treatable by trained clinicians, even in resource-limited settings.
Scabies
Scabies is a parasitic skin infestation caused by the 8-legged mite Sarcoptes scabiei var hominis. The female mite begins the infestation process via penetration of the epidermis, particularly the stratum corneum, and commences laying eggs (Figure 1). The subsequent larvae emerge 48 to 72 hours later and remain burrowed in the epidermis. The larvae mature over the next 10 to 14 days and continue the reproductive cycle.14,15 Symptoms of infestation occurs due to a hypersensitivity reaction to the mite and its by-products.16 Transmission of the mite primarily occurs via direct (skin-to-skin) contact with infected individuals or environmental surfaces for 24 to36 hours in specific conditions, though the latter source has been debated in the literature.
The method of transmission is particularly important when considering care for refugee populations. Scabies is found most often in those living in or traveling from tropical regions including East Asia, Southeast Asia, Oceania, and Latin America.17 In displaced or refugee populations, a lack of access to basic hygiene, extended travel in close quarters, and suboptimal health care access all may lead to an increased incidence of untreated scabies infestations.18 Scabies is more prevalent in children, with increased potential for secondary bacterial infections with Streptococcus and Staphylococcus species due to excoriation in unsanitary conditions. Secondary infection with Streptococcus pyogenes can lead to acute poststreptococcal glomerulonephritis, which accounts for a large burden of chronic kidney disease in affected populations.19 However, scabies may be found in any population, regardless of hygiene or health care access. Treating health care providers should keep a broad differential.
Presentation—The latency of scabies symptoms is 2 to 6 weeks in a primary outbreak and may be as short as 1 to 3 days with re-infestation, following the course of delayed-type hypersensitivity.20 The initial hallmark symptom is pruritus with increased severity in the evening. Visible lesions, excoriations, and burrows associated with scattered vesicles or pustules may be seen over the web spaces of the hands and feet, volar surfaces of the wrists, axillae, waist, genitalia, inner thighs, or buttocks.19 Chronic infestation often manifests with genital nodules. In populations with limited access to health care, there are reports of a sensitization phenomenon in which the individual may become less symptomatic after 4 to 6 weeks and yet be a potential carrier of the mite.21
Those with compromised immune function, such as individuals living with HIV or severe malnutrition, may present with crusted scabies, a variant that manifests as widespread hyperkeratotic scaling with more pronounced involvement of the head, neck, and acral areas. In contrast to classic scabies, crusted scabies is associated with minimal pruritus.22
Diagnosis—The diagnosis of scabies is largely clinical with confirmation through skin scrapings. The International Alliance for Control of Scabies has established diagnostic criteria that include a combination of clinical findings, history, and visualization of mites.23 A dermatologist working with refugee populations may employ any combination of history (eg, nocturnal itch, exposure to an affected individual) or clinical findings along with a high degree of suspicion in those with elevated risk. Visualization of mites is helpful to confirm the diagnosis and may be completed with the application of mineral oil at the terminal end of a burrow, skin scraping with a surgical blade or needle, and examination under light microscopy.
Treatment—First-line treatment for scabies consists of application of permethrin cream 5% on the skin of the neck to the soles of the feet, which is to be left on for 8 to 14 hours followed by rinsing. Re-application is recommended in 1 to 2 weeks. Oral ivermectin is a reasonable alternative to permethrin cream due to its low cost and easy administration in large affected groups. It is not labeled for use in pregnant women or children weighing less than 15 kg but has no selective fetal toxicity. Treatment of scabies with ivermectin has the benefit of treating many other parasitic infections. Both medications are on the World Health Organization Model List of Essential Medications and are widely available for treating providers, even in resource-limited settings.24
Much of the world still uses benzyl benzoate or precipitated sulfur ointment to treat scabies, and some botanicals used in folk medicine have genuine antiscabetic properties. Pruritus may persist for 1 to 4 weeks following treatment and does not indicate treatment failure. Topical camphor and menthol preparations, low-potency topical corticosteroids, or emollients all may be employed for relief.25Sarna is a Spanish term for scabies and has become the proprietary name for topical antipruritic agents. Additional methods of treatment and prevention include washing clothes and linens in hot water and drying on high heat. If machine washing is not available, clothing and linens may be sealed in a plastic bag for 72 hours.
Pediculosis
Pediculosis is an infestation caused by the ectoparasite Pediculus humanus, an obligate, sesame seed–sized louse that feeds exclusively on the blood of its host (Figure 2).26 Of the lice species, 2 require humans as hosts; one is P humanus and the other is Pthirus pubis (pubic lice). Pediculus humanus may be further classified into morphologies based largely on the affected area: body (P humanus corporis) or head (P humanus capitis), both of which will be discussed.27
Lice primarily attach to clothing and hair shafts, then transfer to the skin for blood feeds. Females lay eggs that hatch 6 to 10 days later, subsequently maturing into adults. The lifespan of these parasites with regular access to a host is 1 to 3 months for head lice and 18 days for body lice vs only 3 to 5 days without a host.28 Transmission of P humanus capitis primarily occurs via direct contact with affected individuals, either head-to-head contact or sharing of items such as brushes and headscarves; P humanus corporis also may be transmitted via direct contact with affected individuals or clothing.
Pediculosis is an important infestation to consider when providing care for refugee populations. Risk factors include lack of access to basic hygiene, including regular bathing or laundering of clothing, and crowded conditions that make direct person-to-person contact with affected individuals more likely.29 Body lice are associated more often with domestic turbulence and displaced populations30 in comparison to head lice, which have broad demographic variables, most often affecting females and children.28 Fatty acids in adult male sebum make the scalp less hospitable to lice.
Presentation—The most common clinical manifestation of pediculosis is pruritus. Cutaneous findings can include papules, wheals, or hemorrhagic puncta secondary to the louse bite. Due to the Tyndall effect of deep hemosiderin pigment, blue-grey macules termed maculae ceruleae (Figure 3) also may be present in chronic infestations of pediculosis pubis, in contrast to pediculosis capitis or corporis.31 Body louse infestation is associated with a general pruritus concentrated on the neck, shoulders, and waist—areas where clothing makes the most direct contact. Lesions may be visible and include eczematous patches with excoriation and possible secondary bacterial infection. Chronic infestation may exhibit lichenification or hyperpigmentation in associated areas. Head lice most often manifest with localized scalp pruritus and associated excoriation and cervical or occipital lymphadenopathy.32
Diagnosis—The diagnosis of pediculosis is clinical, with confirmation requiring direct examination of the insect or nits (the egg case of the parasite)(Figure 4). Body lice and associated nits can be visualized on clothing seams near areas of highest body temperature, particularly the waistband. Head lice may be visualized crawling on hair shafts or on a louse comb. Nits are firmly attached to hair shafts and are visible to the naked eye, whereas pseudonits slide freely along the hair shaft and are not a manifestation of louse infestation (Figure 5).31
Treatment—Treatment varies by affected area. Pediculosis corporis may be treated with permethrin cream 5% applied to the entire body and left on for 8 to 10 hours, but this may not be necessary if facilities are available to wash and dry clothing.33 The use of oral ivermectin and permethrin-impregnated underwear both have been proposed.34,35 Treatment of pediculosis capitis may be accomplished with a variety of topical pediculicides including permethrin, pyrethrum with piperonyl butoxide, dimethicone, malathion, benzyl alcohol, spinosad, and topical ivermectin.22 Topical corticosteroids or emollients may be employed for residual pruritus.
Equally important is environmental elimination of infestation. Clothing should be discarded if possible or washed and dried using high heat. If neither approach is possible or appropriate, clothing may be sealed in a plastic bag for 2 weeks or treated with a pediculicide. Nit combing is an important adjunct in the treatment of pediculosis capitis.36 It is important to encourage return to work and/or school immediately after treatment. “No nit” policies are more harmful to education than helpful for prevention of investation.37
Pediculosis corporis may transmit infectious agents including Bartonella quintana, (trench fever, endocarditis, bacillary angiomatosis), Borrelia recurrentis (louse-borne relapsing fever), and Rickettsia prowazekii (epidemic typhus).31,38,39 Additionally, severe pediculosis infestations have the potential to cause chronic blood loss in affected populations. In a study of patients with active pediculosis infestation, mean hemoglobin values were found to be 2.5 g/dL lower than a matched population without infestation.40 It is important to consider pediculosis as a risk for iron-deficiency anemia in populations who are known to lack access to regular medical evaluation.41
Future Considerations
Increased access to tools and education for clinicians treating refugee populations is key to reducing the burden of parasitic skin disease and related morbidity and mortality in vulnerable groups both domestically and globally. One such tool, the Skin NTDs App, was launched by the World Health Organization in 2020. It is available for free for Android and iOS devices to assist clinicians in the field with the diagnosis and treatment of neglected tropical diseases—including scabies—that may affect refugee populations.42
Additionally, to both improve access and limit preventable sequelae, future investigations into appropriate models of community-based care are paramount. The model of community-based care is centered on the idea of care provision that prioritizes safety, accessibility, affordability, and acceptability in an environment closest to vulnerable populations. The largest dermatologic society, the International League of Dermatological Societies, formed a Migrant Health Dermatology Working Group that prioritizes understanding and improving care for refugee and migrant populations; this group hosted a summit in 2022, bringing together international subject matter leaders to discuss such models of care and set goals for the creation of tool kits for patients, frontline health care workers, and dermatologists.43
Conclusion
Improvement in dermatologic care of refugee populations includes provision of culturally and linguistically appropriate care by trained clinicians, adequate access to the most essential medications, and basic physical or legal access to health care systems in general.8,11,44 Parasitic infestations have the potential to remain asymptomatic for extended periods of time and result in spread to potentially nonendemic regions of resettlement.45 Additionally, the psychosocial well-being of refugee populations upon resettlement may be negatively affected by stigma of disease processes such as scabies and pediculosis, leading to additional barriers to successful re-entry into the patient’s new environment.46 Therefore, proper screening, diagnosis, and treatment of the most common parasitic infestations in this population have great potential to improve outcomes for large groups across the globe.
- Monin K, Batalova J, Lai T. Refugees and Asylees in the United States. Migration Information Source. Published May 13, 2021. Accessed April 4, 2024. https://www.migrationpolicy.org/article/refugees-and-asylees-united-states-2021
- UNHCR. Figures at a Glance. UNHCR USA. Update June 14, 2023. Accessed April 4, 2024. https://www.unhcr.org/en-us/figures-at-a-glance.html
- UNHCR. Refugee resettlement facts. Published October 2023. Accessed April 8, 2024. https://www.unhcr.org/us/media/refugee-resettlement-facts
- US Department of State. Report to Congress on Proposed Refugee Admissions for Fiscal Year 2024. Published November 3, 2023. Accessed April 8, 2024. https://www.state.gov/report-to-congress-on-proposed-refugee-admissions-for-fiscal-year-2024/
- UNHCR. Compact for Migration: Definitions. United Nations. Accessed April 4, 2024. https://refugeesmigrants.un.org/definitions
- United Nations High Commissioner for Refugees (UNHCR). Convention and Protocol Relating to the Status of Refugees. Published December 2010. Accessed January 11, 2024. https://www.unhcr.org/us/media/convention-and-protocol-relating-status-refugees
- Kibar Öztürk M. Skin diseases in rural Nyala, Sudan (in a rural hospital, in 12 orphanages, and in two refugee camps). Int J Dermatol. 2019;58:1341-1349. doi:10.1111/ijd.14619
- Padovese V, Knapp A. Challenges of managing skin diseases in refugees and migrants. Dermatol Clin. 2021;39:101-115. doi:10.1016/j.det.2020.08.010
- Saikal SL, Ge L, Mir A, et al. Skin disease profile of Syrian refugees in Jordan: a field-mission assessment. J Eur Acad Dermatol Venereol. 2020;34:419-425. doi:10.1111/jdv.15909
- Eonomopoulou A, Pavli A, Stasinopoulou P, et al. Migrant screening: lessons learned from the migrant holding level at the Greek-Turkish borders. J Infect Public Health. 2017;10:177-184. doi:10.1016/j.jiph.2016.04.012
- Marano N, Angelo KM, Merrill RD, et al. Expanding travel medicine in the 21st century to address the health needs of the world’s migrants.J Travel Med. 2018;25. doi:10.1093/jtm/tay067
- Hay RJ, Asiedu K. Skin-related neglected tropical diseases (skin NTDs)—a new challenge. Trop Med Infect Dis. 2018;4. doi:10.3390/tropicalmed4010004
- NIAID. Neglected tropical diseases. Updated July 11, 2016. Accessed April 4, 2024. https://www.niaid.nih.gov/research/neglected-tropical-diseases
- Arlian LG, Morgan MS. A review of Sarcoptes scabiei: past, present and future. Parasit Vectors. 2017;10:297. doi:10.1186/s13071-017-2234-1
- Arlian LG, Runyan RA, Achar S, et al. Survival and infectivity of Sarcoptes scabiei var. canis and var. hominis. J Am Acad Dermatol. 1984;11(2 pt 1):210-215. doi:10.1016/s0190-9622(84)70151-4
- Chandler DJ, Fuller LC. A review of scabies: an infestation more than skin deep. Dermatology. 2019;235:79-90. doi:10.1159/000495290
- Karimkhani C, Colombara DV, Drucker AM, et al. The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17:1247-1254. doi:10.1016/S1473-3099(17)30483-8
- Romani L, Steer AC, Whitfeld MJ, et al. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet Infect Dis. 2015;15:960-967. doi:10.1016/S1473-3099(15)00132-2
- Thomas C, Coates SJ, Engelman D, et al. Ectoparasites: scabies. J Am Acad Dermatol. 2020;82:533-548. doi:10.1016/j.jaad.2019.05.109
- Mellanby K, Johnson CG, Bartley WC. Treatment of scabies. Br Med J. 1942;2:1-4. doi:10.1136/bmj.2.4252.1
- Walton SF. The immunology of susceptibility and resistance to scabies. Parasit Immunol. 2010;32:532-540. doi:10.1111/j.1365-3024.2010.01218.x
- Coates SJ, Thomas C, Chosidow O, et al. Ectoparasites: pediculosis and tungiasis. J Am Acad Dermatol. 2020;82:551-569. doi:10.1016/j.jaad.2019.05.110
- Engelman D, Fuller LC, Steer AC; International Alliance for the Control of Scabies Delphi p. Consensus criteria for the diagnosis of scabies: a Delphi study of international experts. PLoS Negl Trop Dis. 2018;12:E0006549. doi:10.1371/journal.pntd.0006549
- World Health Organization. WHO Model Lists of Essential Medicines—23rd list, 2023. Updated July 26, 2023. Accessed April 8, 2024. https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Badiaga S, Brouqui P. Human louse-transmitted infectious diseases. Clin Microbiol Infect. 2012;18:332-337. doi:10.1111/j.1469-0691.2012.03778.x
- Leo NP, Campbell NJH, Yang X, et al. Evidence from mitochondrial DNA that head lice and body lice of humans (Phthiraptera: Pediculidae) are conspecific. J Med Entomol. 2002;39:662-666. doi:10.1603/0022-2585-39.4.662
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826. doi:10.1016/S0140-6736(99)09458-1
- Arnaud A, Chosidow O, Détrez M-A, et al. Prevalences of scabies and pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112. doi:10.1111/bjd.14226
- Brouqui P. Arthropod-borne diseases associated with political and social disorder. Annu Rev Entomol. 2011;56:357-374. doi:10.1146/annurev-ento-120709-144739
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12. doi:10.1016/S0190-9622(03)02729-4
- Bloomfield D. Head lice. Pediatr Rev. 2002;23:34-35; discussion 34-35. doi:10.1542/pir.23-1-34
- Stone SP GJ, Bacelieri RE. Scabies, other mites, and pediculosis. In: Wolf K GL, Katz SI, et al (eds). Fitzpatrick’s Dermatology in General Medicine. McGraw Hill; 2008:2029.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476. doi:10.1086/499279
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279. doi:10.1001/jamadermatol.2013.6398
- CDC. Parasites: Treatment. Updated October 15, 2019. Accessed April 4, 2024. https://www.cdc.gov/parasites/lice/head/treatment.html
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:e1355-e1365. doi:10.1542/peds.2015-0746
- Ohl ME, Spach DH. Bartonella quintana and urban trench fever. Clin Infect Dis. 2000;31:131-135. doi:10.1086/313890
- Drali R, Sangaré AK, Boutellis A, et al. Bartonella quintana in body lice from scalp hair of homeless persons, France. Emerg Infect Dis. 2014;20:907-908. doi:10.3201/eid2005.131242
- Rudd N, Zakaria A, Kohn MA, et al. Association of body lice infestation with hemoglobin values in hospitalized dermatology patients. JAMA Dermatol. 2022;158:691-693. doi:10.1001/jamadermatol.2022.0818
- Guss DA, Koenig M, Castillo EM. Severe iron deficiency anemia and lice infestation. J Emergency Med. 2011;41:362-365. doi:10.1016/j.jemermed.2010.05.030
- Neglected tropical diseases of the skin: WHO launches mobile application to facilitate diagnosis. News release. World Health Organization; July 16, 2020. Accessed April 4, 2024. https://www.who.int/news/item/16-07-2020-neglected-tropical-diseases-of-the-skin-who-launches-mobile-application-to-facilitate-diagnosis
- Padovese V, Fuller LC, Griffiths CEM, et al; Migrant Health Dermatology Working Group of the International Foundation for Dermatology. Migrant skin health: perspectives from the Migrant Health Summit, Malta, 2022. Br J Dermatology. 2023;188:553-554. doi:10.1093/bjd/ljad001
- Knapp AP, Rehmus W, Chang AY. Skin diseases in displaced populations: a review of contributing factors, challenges, and approaches to care. Int J Dermatol. 2020;59:1299-1311. doi:10.1111/ijd.15063
- Norman FF, Comeche B, Chamorro S, et al. Overcoming challenges in the diagnosis and treatment of parasitic infectious diseases in migrants. Expert Rev Anti-infective Therapy. 2020;18:127-143. doi:10.1080/14787210.2020.1713099
- Skin NTDs: prioritizing integrated approaches to reduce suffering, psychosocial impact and stigmatization. News release. World Health Organization; October 29, 2020. Accessed April 4, 2024. https://www.who.int/news/item/29-10-2020-skin-ntds-prioritizing-integrated-approaches-to-reduce-suffering-psychosocial-impact-and-stigmatization
- Monin K, Batalova J, Lai T. Refugees and Asylees in the United States. Migration Information Source. Published May 13, 2021. Accessed April 4, 2024. https://www.migrationpolicy.org/article/refugees-and-asylees-united-states-2021
- UNHCR. Figures at a Glance. UNHCR USA. Update June 14, 2023. Accessed April 4, 2024. https://www.unhcr.org/en-us/figures-at-a-glance.html
- UNHCR. Refugee resettlement facts. Published October 2023. Accessed April 8, 2024. https://www.unhcr.org/us/media/refugee-resettlement-facts
- US Department of State. Report to Congress on Proposed Refugee Admissions for Fiscal Year 2024. Published November 3, 2023. Accessed April 8, 2024. https://www.state.gov/report-to-congress-on-proposed-refugee-admissions-for-fiscal-year-2024/
- UNHCR. Compact for Migration: Definitions. United Nations. Accessed April 4, 2024. https://refugeesmigrants.un.org/definitions
- United Nations High Commissioner for Refugees (UNHCR). Convention and Protocol Relating to the Status of Refugees. Published December 2010. Accessed January 11, 2024. https://www.unhcr.org/us/media/convention-and-protocol-relating-status-refugees
- Kibar Öztürk M. Skin diseases in rural Nyala, Sudan (in a rural hospital, in 12 orphanages, and in two refugee camps). Int J Dermatol. 2019;58:1341-1349. doi:10.1111/ijd.14619
- Padovese V, Knapp A. Challenges of managing skin diseases in refugees and migrants. Dermatol Clin. 2021;39:101-115. doi:10.1016/j.det.2020.08.010
- Saikal SL, Ge L, Mir A, et al. Skin disease profile of Syrian refugees in Jordan: a field-mission assessment. J Eur Acad Dermatol Venereol. 2020;34:419-425. doi:10.1111/jdv.15909
- Eonomopoulou A, Pavli A, Stasinopoulou P, et al. Migrant screening: lessons learned from the migrant holding level at the Greek-Turkish borders. J Infect Public Health. 2017;10:177-184. doi:10.1016/j.jiph.2016.04.012
- Marano N, Angelo KM, Merrill RD, et al. Expanding travel medicine in the 21st century to address the health needs of the world’s migrants.J Travel Med. 2018;25. doi:10.1093/jtm/tay067
- Hay RJ, Asiedu K. Skin-related neglected tropical diseases (skin NTDs)—a new challenge. Trop Med Infect Dis. 2018;4. doi:10.3390/tropicalmed4010004
- NIAID. Neglected tropical diseases. Updated July 11, 2016. Accessed April 4, 2024. https://www.niaid.nih.gov/research/neglected-tropical-diseases
- Arlian LG, Morgan MS. A review of Sarcoptes scabiei: past, present and future. Parasit Vectors. 2017;10:297. doi:10.1186/s13071-017-2234-1
- Arlian LG, Runyan RA, Achar S, et al. Survival and infectivity of Sarcoptes scabiei var. canis and var. hominis. J Am Acad Dermatol. 1984;11(2 pt 1):210-215. doi:10.1016/s0190-9622(84)70151-4
- Chandler DJ, Fuller LC. A review of scabies: an infestation more than skin deep. Dermatology. 2019;235:79-90. doi:10.1159/000495290
- Karimkhani C, Colombara DV, Drucker AM, et al. The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17:1247-1254. doi:10.1016/S1473-3099(17)30483-8
- Romani L, Steer AC, Whitfeld MJ, et al. Prevalence of scabies and impetigo worldwide: a systematic review. Lancet Infect Dis. 2015;15:960-967. doi:10.1016/S1473-3099(15)00132-2
- Thomas C, Coates SJ, Engelman D, et al. Ectoparasites: scabies. J Am Acad Dermatol. 2020;82:533-548. doi:10.1016/j.jaad.2019.05.109
- Mellanby K, Johnson CG, Bartley WC. Treatment of scabies. Br Med J. 1942;2:1-4. doi:10.1136/bmj.2.4252.1
- Walton SF. The immunology of susceptibility and resistance to scabies. Parasit Immunol. 2010;32:532-540. doi:10.1111/j.1365-3024.2010.01218.x
- Coates SJ, Thomas C, Chosidow O, et al. Ectoparasites: pediculosis and tungiasis. J Am Acad Dermatol. 2020;82:551-569. doi:10.1016/j.jaad.2019.05.110
- Engelman D, Fuller LC, Steer AC; International Alliance for the Control of Scabies Delphi p. Consensus criteria for the diagnosis of scabies: a Delphi study of international experts. PLoS Negl Trop Dis. 2018;12:E0006549. doi:10.1371/journal.pntd.0006549
- World Health Organization. WHO Model Lists of Essential Medicines—23rd list, 2023. Updated July 26, 2023. Accessed April 8, 2024. https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02
- Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. J Eur Acad Dermatol Venereol. 2017;31:1248-1253. doi:10.1111/jdv.14351
- Badiaga S, Brouqui P. Human louse-transmitted infectious diseases. Clin Microbiol Infect. 2012;18:332-337. doi:10.1111/j.1469-0691.2012.03778.x
- Leo NP, Campbell NJH, Yang X, et al. Evidence from mitochondrial DNA that head lice and body lice of humans (Phthiraptera: Pediculidae) are conspecific. J Med Entomol. 2002;39:662-666. doi:10.1603/0022-2585-39.4.662
- Chosidow O. Scabies and pediculosis. Lancet. 2000;355:819-826. doi:10.1016/S0140-6736(99)09458-1
- Arnaud A, Chosidow O, Détrez M-A, et al. Prevalences of scabies and pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). Br J Dermatol. 2016;174:104-112. doi:10.1111/bjd.14226
- Brouqui P. Arthropod-borne diseases associated with political and social disorder. Annu Rev Entomol. 2011;56:357-374. doi:10.1146/annurev-ento-120709-144739
- Ko CJ, Elston DM. Pediculosis. J Am Acad Dermatol. 2004;50:1-12. doi:10.1016/S0190-9622(03)02729-4
- Bloomfield D. Head lice. Pediatr Rev. 2002;23:34-35; discussion 34-35. doi:10.1542/pir.23-1-34
- Stone SP GJ, Bacelieri RE. Scabies, other mites, and pediculosis. In: Wolf K GL, Katz SI, et al (eds). Fitzpatrick’s Dermatology in General Medicine. McGraw Hill; 2008:2029.
- Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. J Infect Dis. 2006;193:474-476. doi:10.1086/499279
- Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. JAMA Dermatol. 2014;150:273-279. doi:10.1001/jamadermatol.2013.6398
- CDC. Parasites: Treatment. Updated October 15, 2019. Accessed April 4, 2024. https://www.cdc.gov/parasites/lice/head/treatment.html
- Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. Pediatrics. 2015;135:e1355-e1365. doi:10.1542/peds.2015-0746
- Ohl ME, Spach DH. Bartonella quintana and urban trench fever. Clin Infect Dis. 2000;31:131-135. doi:10.1086/313890
- Drali R, Sangaré AK, Boutellis A, et al. Bartonella quintana in body lice from scalp hair of homeless persons, France. Emerg Infect Dis. 2014;20:907-908. doi:10.3201/eid2005.131242
- Rudd N, Zakaria A, Kohn MA, et al. Association of body lice infestation with hemoglobin values in hospitalized dermatology patients. JAMA Dermatol. 2022;158:691-693. doi:10.1001/jamadermatol.2022.0818
- Guss DA, Koenig M, Castillo EM. Severe iron deficiency anemia and lice infestation. J Emergency Med. 2011;41:362-365. doi:10.1016/j.jemermed.2010.05.030
- Neglected tropical diseases of the skin: WHO launches mobile application to facilitate diagnosis. News release. World Health Organization; July 16, 2020. Accessed April 4, 2024. https://www.who.int/news/item/16-07-2020-neglected-tropical-diseases-of-the-skin-who-launches-mobile-application-to-facilitate-diagnosis
- Padovese V, Fuller LC, Griffiths CEM, et al; Migrant Health Dermatology Working Group of the International Foundation for Dermatology. Migrant skin health: perspectives from the Migrant Health Summit, Malta, 2022. Br J Dermatology. 2023;188:553-554. doi:10.1093/bjd/ljad001
- Knapp AP, Rehmus W, Chang AY. Skin diseases in displaced populations: a review of contributing factors, challenges, and approaches to care. Int J Dermatol. 2020;59:1299-1311. doi:10.1111/ijd.15063
- Norman FF, Comeche B, Chamorro S, et al. Overcoming challenges in the diagnosis and treatment of parasitic infectious diseases in migrants. Expert Rev Anti-infective Therapy. 2020;18:127-143. doi:10.1080/14787210.2020.1713099
- Skin NTDs: prioritizing integrated approaches to reduce suffering, psychosocial impact and stigmatization. News release. World Health Organization; October 29, 2020. Accessed April 4, 2024. https://www.who.int/news/item/29-10-2020-skin-ntds-prioritizing-integrated-approaches-to-reduce-suffering-psychosocial-impact-and-stigmatization
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>Strahan</fileName> <TBEID>0C02F581.SIG</TBEID> <TBUniqueIdentifier>NJ_0C02F581</TBUniqueIdentifier> <newsOrJournal>Journal</newsOrJournal> <publisherName>Frontline Medical Communications Inc.</publisherName> <storyname>Clinical Review</storyname> <articleType>1</articleType> <TBLocation>Published-CT</TBLocation> <QCDate/> <firstPublished>20240425T131253</firstPublished> <LastPublished>20240425T132642</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240425T131253</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Strahan</byline> <bylineText>Alexis G. Strahan, MD, MSN; Dirk M. Elston, MD</bylineText> <bylineFull>Strahan</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange>E16-E21</pageRange> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:"> <name/> <rightsInfo> <copyrightHolder> <name/> </copyrightHolder> <copyrightNotice/> </rightsInfo> </provider> <abstract/> <metaDescription>Approximately 108 million individuals have been forcibly displaced across the globe as of 2022, 35 million of whom are formally designated as refugees.1,2 The U</metaDescription> <articlePDF>301172</articlePDF> <teaserImage/> <title>Dermatologic Care for Refugees: Effective Management of Scabies and Pediculosis</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>2</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear>2024</pubPubdateYear> <pubPubdateMonth>April</pubPubdateMonth> <pubPubdateDay/> <pubVolume>113</pubVolume> <pubNumber>4</pubNumber> <wireChannels/> <primaryCMSID/> <CMSIDs> <CMSID>2293</CMSID> <CMSID>2161</CMSID> </CMSIDs> <keywords> <keyword>infectious disease</keyword> <keyword> scabies</keyword> <keyword> pediculosis</keyword> </keywords> <seeAlsos/> <publications_g> <publicationData> <publicationCode>CT</publicationCode> <pubIssueName>April 2024</pubIssueName> <pubArticleType>Original Articles | 2161</pubArticleType> <pubTopics/> <pubCategories/> <pubSections> <pubSection>Original Article | 2293<pubSubsection/></pubSection> </pubSections> <journalTitle>Cutis</journalTitle> <journalFullTitle>Cutis</journalFullTitle> <copyrightStatement>Copyright 2015 Frontline Medical Communications Inc., Parsippany, NJ, USA. All rights reserved.</copyrightStatement> </publicationData> </publications_g> <publications> <term canonical="true">12</term> </publications> <sections> <term canonical="true">49</term> </sections> <topics> <term canonical="true">234</term> </topics> <links> <link> <itemClass qcode="ninat:composite"/> <altRep contenttype="application/pdf">images/1800270f.pdf</altRep> <description role="drol:caption"/> <description role="drol:credit"/> </link> </links> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Dermatologic Care for Refugees: Effective Management of Scabies and Pediculosis</title> <deck/> </itemMeta> <itemContent> <p class="abstract">There is a large burden of treatable dermatologic conditions in refugee populations. Parasitic infestations are particularly common when there are barriers to basic hygiene, crowded living or travel conditions, and lack of access to health care. Body lice are associated with anemia and can transmit a variety of diseases; chronic impetigo secondary to scabies is a leading cause of chronic kidney disease globally. Dermatologists have unique skills to identify skin infections, inflammatory diseases, and infestations. Appropriate dermatologic care has the potential to improve overall outcomes.</p> <p>Approximately 108 million individuals have been forcibly displaced across the globe as of 2022, 35 million of whom are formally designated as refugees.<sup>1,2</sup> The United States has coordinated resettlement of more refugee populations than any other country; the most common countries of origin are the Democratic Republic of the Congo, Syria, Afghanistan, and Myanmar.<sup>3</sup> In 2021, policy to increase the number of refugees resettled in the United States by more than 700% (from 15,000 up to 125,000) was established; since enactment, the United States has seen more than double the refugee arrivals in 2023 than the prior year, making medical care for this population increasingly relevant for the dermatologist.<sup>4</sup> </p> <p>Understanding how to care for this population begins with an accurate understanding of the term <i>refugee</i>. The United Nations defines a refugee as a person who is unwilling or unable to return to their country of nationality because of persecution or well-founded fear of persecution due to race, religion, nationality, membership in a particular social group, or political opinion. This term grants a protected status under international law and encompasses access to travel assistance, housing, cultural orientation, and medical evaluation upon resettlement.<sup>5,6</sup> <br/><br/>The burden of treatable dermatologic conditions in refugee populations ranges from 19% to 96% in the literature<sup>7,8</sup> and varies from inflammatory disorders to infectious and parasitic diseases.<sup>9</sup> In one study of 6899 displaced individuals in Greece, the prevalence of dermatologic conditions was higher than traumatic injury, cardiac disease, psychological conditions, and dental disease.<sup>10</sup> <br/><br/>When outlining differential diagnoses for parasitic infestations of the skin that affect refugee populations, helpful considerations include the individual’s country of origin, route traveled, and method of travel.<sup>11</sup> Parasitic infestations specifically are more common in refugee populations when there are barriers to basic hygiene, crowded living or travel conditions, or lack of access to health care, which they may experience at any point in their home country, during travel, or in resettlement housing.<sup>8</sup> <br/><br/>Even with limited examination and diagnostic resources, the skin is the most accessible first indication of patients’ overall well-being and often provides simple diagnostic clues—in combination with contextualization of the patient’s unique circumstances—necessary for successful diagnosis and treatment of scabies and pediculosis.<sup>12</sup> The dermatologist working with refugee populations may be the first set of eyes available and trained to discern skin infestations and therefore has the potential to improve overall outcomes. <br/><br/>Some parasitic infestations in refugee populations may fall under the category of neglected tropical diseases, including scabies, ascariasis, trypanosomiasis, leishmaniasis, and schistosomiasis; they affect an estimated 1 billion individuals across the globe but historically have been underrepresented in the literature and in health policy due in part to limited access to care.<sup>13</sup> This review will focus on infestations by the scabies mite (<i>Sarcoptes scabiei </i>var <i>hominis</i>)<i> </i>and the human louse, as these frequently are encountered, easily diagnosed, and treatable by trained clinicians, even in resource-limited settings. </p> <h3>Scabies </h3> <p>Scabies is a parasitic skin infestation caused by the 8-legged mite <i>Sarcoptes scabiei </i>var<i> hominis.</i> The female mite begins the infestation process via penetration of the epidermis, particularly the stratum corneum, and commences laying eggs (Figure 1). The subsequent larvae emerge 48 to 72 hours later and remain burrowed in the epidermis. The larvae mature over the next 10 to 14 days and continue the reproductive cycle.<sup>14,15</sup> Symptoms of infestation occurs due to a hypersensitivity reaction to the mite and its by-products.<sup>16</sup> Transmission of the mite primarily occurs via direct (skin-to-skin) contact with infected individuals or environmental surfaces for 24 to36 hours in specific conditions, though the latter source has been debated in the literature. </p> <p>The method of transmission is particularly important when considering care for refugee populations. Scabies is found most often in those living in or traveling from tropical regions including East Asia, Southeast Asia, Oceania, and Latin America.<sup>17</sup> In displaced or refugee populations, a lack of access to basic hygiene, extended travel in close quarters, and suboptimal health care access all may lead to an increased incidence of untreated scabies infestations.<sup>18</sup> Scabies is more prevalent in children, with increased potential for secondary bacterial infections with <i>Streptococcus</i> and <i>Staphylococcus</i> species due to excoriation in unsanitary conditions. Secondary infection with <i>Streptococcus pyogenes</i> can lead to acute poststreptococcal glomerulonephritis, which accounts for a large burden of chronic kidney disease in affected populations.<sup>19</sup> However, scabies may be found in any population, regardless of hygiene or health care access. Treating health care providers should keep a broad differential. <br/><br/><i>Presentation—</i>The latency of scabies symptoms is 2 to 6 weeks in a primary outbreak and may be as short as 1 to 3 days with re-infestation, following the course of delayed-type hypersensitivity.<sup>20</sup> The initial hallmark symptom is pruritus with increased severity in the evening. Visible lesions, excoriations, and burrows associated with scattered vesicles or pustules may be seen over the web spaces of the hands and feet, volar surfaces of the wrists, axillae, waist, genitalia, inner thighs, or buttocks.<sup>19</sup> Chronic infestation often manifests with genital nodules. In populations with limited access to health care, there are reports of a sensitization phenomenon in which the individual may become less symptomatic after 4 to 6 weeks and yet be a potential carrier of the mite.<sup>21</sup><i> <br/><br/></i>Those with compromised immune function, such as individuals living with HIV or severe malnutrition, may present with crusted scabies, a variant that manifests as widespread hyperkeratotic scaling with more pronounced involvement of the head, neck, and acral areas. In contrast to classic scabies, crusted scabies is associated with minimal pruritus.<sup>22</sup> <br/><br/><i>Diagnosis—</i>The diagnosis of scabies is largely clinical with confirmation through skin scrapings. The International Alliance for Control of Scabies has established diagnostic criteria that include a combination of clinical findings, history, and visualization of mites.<sup>23</sup> A dermatologist working with refugee populations may employ any combination of history (eg, nocturnal itch, exposure to an affected individual) or clinical findings along with a high degree of suspicion in those with elevated risk. Visualization of mites is helpful to confirm the diagnosis and may be completed with the application of mineral oil at the terminal end of a burrow, skin scraping with a surgical blade or needle, and examination under light microscopy. <br/><br/><i>Treatment—</i>First-line treatment for scabies consists of application of permethrin cream 5% on the skin of the neck to the soles of the feet, which is to be left on for 8 to 14 hours followed by rinsing. Re-application is recommended in 1 to 2 weeks. Oral ivermectin is a reasonable alternative to permethrin cream due to its low cost and easy administration in large affected groups. It is not labeled for use in pregnant women or children weighing less than 15 kg but has no selective fetal toxicity. Treatment of scabies with ivermectin has the benefit of treating many other parasitic infections. Both medications are on the <i>World Health Organization Model List of Essential Medications</i> and are widely available for treating providers, even in resource-limited settings.<sup>24</sup> <br/><br/>Much of the world still uses benzyl benzoate or precipitated sulfur ointment to treat scabies, and some botanicals used in folk medicine have genuine antiscabetic properties. Pruritus may persist for 1 to 4 weeks following treatment and does not indicate treatment failure. Topical camphor and menthol preparations, low-potency topical corticosteroids, or emollients all may be employed for relief.<sup>25</sup> <em>Sarna</em> is a Spanish term for scabies and has become the proprietary name for topical antipruritic agents. Additional methods of treatment and prevention include washing clothes and linens in hot water and drying on high heat. If machine washing is not available, clothing and linens may be sealed in a plastic bag for 72 hours. </p> <h3>Pediculosis </h3> <p>Pediculosis is an infestation caused by the ectoparasite <i>Pediculus humanus</i>, an obligate, sesame seed–sized louse that feeds exclusively on the blood of its host (Figure 2).<sup>26</sup> Of the lice species, 2 require humans as hosts; one is <i>P humanus</i> and the other is <i>Pthirus pubis</i> (pubic lice). <i>Pediculus humanus </i>may be further classified into morphologies based largely on the affected area: body (<i>P humanus</i> <i>corporis)</i> or head (<i>P humanus</i> <i>capitis)</i>, both of which will be discussed.<sup>27</sup> </p> <p>Lice primarily attach to clothing and hair shafts, then transfer to the skin for blood feeds. Females lay eggs that hatch 6 to 10 days later, subsequently maturing into adults. The lifespan of these parasites with regular access to a host is 1 to 3 months for head lice and 18 days for body lice vs only 3 to 5 days without a host.<sup>28</sup> Transmission of <i>P humanus capitis </i>primarily occurs via direct contact with affected individuals, either head-to-head contact or sharing of items such as brushes and headscarves; <i>P humanus corporis</i> also may be transmitted via direct contact with affected individuals or clothing. <br/><br/>Pediculosis is an important infestation to consider when providing care for refugee populations. Risk factors include lack of access to basic hygiene, including regular bathing or laundering of clothing, and crowded conditions that make direct person-to-person contact with affected individuals more likely.<sup>29</sup> Body lice are associated more often with domestic turbulence and displaced populations<sup>30</sup> in comparison to head lice, which have broad demographic variables, most often affecting females and children.<sup>28</sup> Fatty acids in adult male sebum make the scalp less hospitable to lice. <br/><br/><i>Presentation</i>—The most common clinical manifestation of pediculosis is pruritus. Cutaneous findings can include papules, wheals, or hemorrhagic puncta secondary to the louse bite. Due to the Tyndall effect of deep hemosiderin pigment, blue-grey macules termed <i>maculae ceruleae</i> (Figure 3) also may be present in chronic infestations of pediculosis pubis, in contrast to pediculosis capitis or corporis.<sup>31</sup> Body louse infestation is associated with a general pruritus concentrated on the neck, shoulders, and waist—areas where clothing makes the most direct contact. Lesions may be visible and include eczematous patches with excoriation and possible secondary bacterial infection. Chronic infestation may exhibit lichenification or hyperpigmentation in associated areas. Head lice most often manifest with localized scalp pruritus and associated excoriation and cervical or occipital lymphadenopathy.<sup>32</sup> <br/><br/><i>Diagnosis—</i>The diagnosis of pediculosis is clinical, with confirmation requiring direct examination of the insect or nits (the egg case of the parasite)(Figure 4). Body lice and associated nits can be visualized on clothing seams near areas of highest body temperature, particularly the waistband. Head lice may be visualized crawling on hair shafts or on a louse comb. Nits are firmly attached to hair shafts and are visible to the naked eye, whereas pseudonits slide freely along the hair shaft and are not a manifestation of louse infestation (Figure 5).<sup>31</sup> <br/><br/><i>Treatment—</i>Treatment varies by affected area. Pediculosis corporis may be treated with permethrin cream 5% applied to the entire body and left on for 8 to 10 hours, but this may not be necessary if facilities are available to wash and dry clothing.<sup>33</sup> The use of oral ivermectin and permethrin-impregnated underwear both have been proposed.<sup>34,35</sup> Treatment of pediculosis capitis may be accomplished with a variety of topical pediculicides including permethrin, pyrethrum with piperonyl butoxide, dimethicone, malathion, benzyl alcohol, spinosad, and topical ivermectin.<sup>22</sup> Topical corticosteroids or emollients may be employed for residual pruritus. <br/><br/>Equally important is environmental elimination of infestation. Clothing should be discarded if possible or washed and dried using high heat. If neither approach is possible or appropriate, clothing may be sealed in a plastic bag for 2 weeks or treated with a pediculicide. Nit combing is an important adjunct in the treatment of pediculosis capitis.<sup>36</sup> It is important to encourage return to work and/or school immediately after treatment. “No nit” policies are more harmful to education than helpful for prevention of investation.<sup>37<br/><br/></sup>Pediculosis corporis may transmit infectious agents including <i>Bartonella quintana</i>, (trench fever, endocarditis, bacillary angiomatosis), <i>Borrelia recurrentis</i> (louse-borne relapsing fever), and <i>Rickettsia prowazekii</i> (epidemic typhus).<sup>31,38,39</sup> Additionally, severe pediculosis infestations have the potential to cause chronic blood loss in affected populations. In a study of patients with active pediculosis infestation, mean hemoglobin values were found to be 2.5 g/dL lower than a matched population without infestation.<sup>40</sup> It is important to consider pediculosis as a risk for iron-deficiency anemia in populations who are known to lack access to regular medical evaluation.<sup>41</sup> </p> <h3>Future Considerations </h3> <p>Increased access to tools and education for clinicians treating refugee populations is key to reducing the burden of parasitic skin disease and related morbidity and mortality in vulnerable groups both domestically and globally. One such tool, the Skin NTDs App, was launched by the World Health Organization in 2020. It is available for free for Android and iOS devices to assist clinicians in the field with the diagnosis and treatment of neglected tropical diseases—including scabies—that may affect refugee populations.<sup>42</sup></p> <p>Additionally, to both improve access and limit preventable sequelae, future investigations into appropriate models of community-based care are paramount. The model of community-based care is centered on the idea of care provision that prioritizes safety, accessibility, affordability, and acceptability in an environment closest to vulnerable populations. The largest dermatologic society, the International League of Dermatological Societies, formed a Migrant Health Dermatology Working Group that prioritizes understanding and improving care for refugee and migrant populations; this group hosted a summit in 2022, bringing together international subject matter leaders to discuss such models of care and set goals for the creation of tool kits for patients, frontline health care workers, and dermatologists.<sup>43</sup></p> <h3>Conclusion</h3> <p>Improvement in dermatologic care of refugee populations includes provision of culturally and linguistically appropriate care by trained clinicians, adequate access to the most essential medications, and basic physical or legal access to health care systems in general.<sup>8,11,44</sup> Parasitic infestations have the potential to remain asymptomatic for extended periods of time and result in spread to potentially nonendemic regions of resettlement.<sup>45</sup> Additionally, the psychosocial well-being of refugee populations upon resettlement may be negatively affected by stigma of disease processes such as scabies and pediculosis, leading to additional barriers to successful re-entry into the patient’s new environment.<sup>46</sup> Therefore, proper screening, diagnosis, and treatment of the most common parasitic infestations in this population have great potential to improve outcomes for large groups across the globe.</p> <h2>References</h2> <p class="reference"> 1. Monin K, Batalova J, Lai T. Refugees and Asylees in the United States. Migration Information Source. Published May 13, 2021. Accessed April 4, 2024. https://www.migrationpolicy.org/article/refugees-and-asylees-united-states-2021<br/><br/> 2. UNHCR. Figures at a Glance. UNHCR USA. Update June 14, 2023. Accessed April 4, 2024. https://www.unhcr.org/en-us/figures-at-a-glance.html<br/><br/> 3. UNHCR. Refugee resettlement facts. Published October 2023. Accessed April 8, 2024. https://www.unhcr.org/us/media/refugee-resettlement-facts<br/><br/> 4. US Department of State. Report to Congress on Proposed Refugee Admissions for Fiscal Year 2024. Published November 3, 2023. Accessed April 8, 2024. https://www.state.gov/report-to-congress-on-proposed-refugee-admissions-for-fiscal-year-2024/ <br/><br/> 5. UNHCR. Compact for Migration: Definitions. United Nations. Accessed April 4, 2024. https://refugeesmigrants.un.org/definitions<br/><br/> 6. United Nations High Commissioner for Refugees (UNHCR). Convention and Protocol Relating to the Status of Refugees. Published December 2010. Accessed January 11, 2024. https://www.unhcr.org/us/media/convention-and-protocol-relating-status-refugees<br/><br/> 7. Kibar Öztürk M. Skin diseases in rural Nyala, Sudan (in a rural hospital, in 12 orphanages, and in two refugee camps). <i>Int J Dermatol</i>. 2019;58:1341-1349. doi:10.1111/ijd.14619<br/><br/> 8. Padovese V, Knapp A. Challenges of managing skin diseases in refugees and migrants. <i>Dermatol Clin</i>. 2021;39:101-115. doi:10.1016/j.det.2020.08.010<br/><br/> 9. Saikal SL, Ge L, Mir A, et al. Skin disease profile of Syrian refugees in Jordan: a field-mission assessment. <i>J Eur Acad Dermatol Venereol.</i> 2020;34:419-425. doi:10.1111/jdv.15909<br/><br/>10. Eonomopoulou A, Pavli A, Stasinopoulou P, et al. Migrant screening: lessons learned from the migrant holding level at the Greek-Turkish borders. <i>J Infect Public Health</i>. 2017;10:177-184. doi:10.1016/j.jiph.2016.04.012<br/><br/>11. Marano N, Angelo KM, Merrill RD, et al. Expanding travel medicine in the 21st century to address the health needs of the world’s migrants.<i>J Travel Med</i>. 2018;25. doi:10.1093/jtm/tay067<br/><br/>12. Hay RJ, Asiedu K. Skin-related neglected tropical diseases (skin NTDs)—a new challenge. <i>Trop Med Infect Dis</i>. 2018;4. doi:10.3390/tropicalmed4010004<br/><br/>13. NIAID. Neglected tropical diseases. Updated July 11, 2016. Accessed April 4, 2024. https://www.niaid.nih.gov/research/neglected-tropical-diseases<br/><br/>14. Arlian LG, Morgan MS. A review of Sarcoptes scabiei: past, present and future. <i>Parasit Vectors</i>. 2017;10:297. doi:10.1186/s13071-017-2234-1<br/><br/>15. Arlian LG, Runyan RA, Achar S, et al. Survival and infectivity of Sarcoptes scabiei var. canis and var. hominis. <i>J Am Acad Dermatol</i>. 1984;11(2 pt 1):210-215. doi:10.1016/s0190-9622(84)70151-4<br/><br/>16. Chandler DJ, Fuller LC. A review of scabies: an infestation more than skin deep. <i>Dermatology</i>. 2019;235:79-90. doi:10.1159/000495290<br/><br/>17. Karimkhani C, Colombara DV, Drucker AM, et al. The global burden of scabies: a cross-sectional analysis from the Global Burden of Disease Study 2015. <i>Lancet Infect Dis</i>. 2017;17:1247-1254. doi:10.1016/S1473-3099(17)30483-8<br/><br/>18. Romani L, Steer AC, Whitfeld MJ, et al. Prevalence of scabies and impetigo worldwide: a systematic review. <i>Lancet Infect Dis</i>. 2015;15:960-967. doi:10.1016/S1473-3099(15)00132-2<br/><br/>19. Thomas C, Coates SJ, Engelman D, et al. Ectoparasites: scabies. <i>J Am Acad Dermatol</i>. 2020;82:533-548. doi:10.1016/j.jaad.2019.05.109<br/><br/>20. Mellanby K, Johnson CG, Bartley WC. Treatment of scabies. <i>Br Med J</i>. 1942;2:1-4. doi:10.1136/bmj.2.4252.1<br/><br/>21. Walton SF. The immunology of susceptibility and resistance to scabies. <i>Parasit Immunol</i>. 2010;32:532-540. doi:10.1111/j.1365-3024.2010.01218.x<br/><br/>22. Coates SJ, Thomas C, Chosidow O, et al. Ectoparasites: pediculosis and tungiasis. <i>J Am Acad Dermatol</i>. 2020;82:551-569. doi:10.1016/j.jaad.2019.05.110</p> <p class="reference">23. Engelman D, Fuller LC, Steer AC; International Alliance for the Control of Scabies Delphi p. Consensus criteria for the diagnosis of scabies: a Delphi study of international experts. <i>PLoS Negl Trop Dis</i>. 2018;12:E0006549. doi:10.1371/journal.pntd.0006549<br/><br/>24. World Health Organization. WHO Model Lists of Essential Medicines—23rd list, 2023. Updated July 26, 2023. Accessed April 8, 2024. https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2023.02 <br/><br/>25. Salavastru CM, Chosidow O, Boffa MJ, et al. European guideline for the management of scabies. <i>J Eur Acad Dermatol Venereol</i>. 2017;31:1248-1253. doi:10.1111/jdv.14351<br/><br/>26. Badiaga S, Brouqui P. Human louse-transmitted infectious diseases. <i>Clin Microbiol Infect</i>. 2012;18:332-337. doi:10.1111/j.1469-0691.2012.03778.x<br/><br/>27. Leo NP, Campbell NJH, Yang X, et al. Evidence from mitochondrial DNA that head lice and body lice of humans (Phthiraptera: Pediculidae) are conspecific. <i>J Med Entomol. </i>2002;39:662-666. doi:10.1603/0022-2585-39.4.662<br/><br/>28. Chosidow O. Scabies and pediculosis. <i>Lancet</i>. 2000;355:819-826. doi:10.1016/S0140-6736(99)09458-1<br/><br/>29. Arnaud A, Chosidow O, Détrez M-A, et al. Prevalences of scabies and pediculosis corporis among homeless people in the Paris region: results from two randomized cross-sectional surveys (HYTPEAC study). <i>Br J Dermatol</i>. 2016;174:104-112. doi:10.1111/bjd.14226<br/><br/>30. Brouqui P. Arthropod-borne diseases associated with political and social disorder. <i>Annu Rev Entomol</i>. 2011;56:357-374. doi:10.1146/annurev-ento-120709-144739<br/><br/>31. Ko CJ, Elston DM. Pediculosis. <i>J Am Acad Dermatol</i>. 2004;50:1-12. doi:10.1016/S0190-9622(03)02729-4<br/><br/>32. Bloomfield D. Head lice. <i>Pediatr Rev</i>. 2002;23:34-35; discussion 34-35. doi:10.1542/pir.23-1-34<br/><br/>33. Stone SP GJ, Bacelieri RE. Scabies, other mites, and pediculosis. In: Wolf K GL, Katz SI, et al (eds). <i>Fitzpatrick’s Dermatology in General Medicine</i>. McGraw Hill; 2008:2029.<br/><br/>34. Foucault C, Ranque S, Badiaga S, et al. Oral ivermectin in the treatment of body lice. <i>J Infect Dis</i>. 2006;193:474-476. doi:10.1086/499279<br/><br/>35. Benkouiten S, Drali R, Badiaga S, et al. Effect of permethrin-impregnated underwear on body lice in sheltered homeless persons: a randomized controlled trial. <i>JAMA Dermatol. </i>2014;150:273-279. doi:10.1001/jamadermatol.2013.6398<br/><br/>36. CDC. Parasites: Treatment. Updated October 15, 2019. Accessed April 4, 2024. https://www.cdc.gov/parasites/lice/head/treatment.html<br/><br/>37. Devore CD, Schutze GE; Council on School Health and Committee on Infectious Diseases, American Academy of Pediatrics. Head lice. <i>Pediatrics</i>. 2015;135:e1355-e1365. doi:10.1542/peds.2015-0746<br/><br/>38. Ohl ME, Spach DH. Bartonella quintana and urban trench fever. <i>Clin Infect Dis</i>. 2000;31:131-135. doi:10.1086/313890<br/><br/>39. Drali R, Sangaré AK, Boutellis A, et al. Bartonella quintana in body lice from scalp hair of homeless persons, France. <i>Emerg Infect Dis</i>. 2014;20:907-908. doi:10.3201/eid2005.131242<br/><br/>40. Rudd N, Zakaria A, Kohn MA, et al. Association of body lice infestation with hemoglobin values in hospitalized dermatology patients. <i>JAMA Dermatol</i>. 2022;158:691-693. doi:10.1001/jamadermatol.2022.0818</p> <p class="reference">41. Guss DA, Koenig M, Castillo EM. Severe iron deficiency anemia and lice infestation. <i>J Emergency Med</i>. 2011;41:362-365. doi:10.1016/j.jemermed.2010.05.030<br/><br/>42. Neglected tropical diseases of the skin: WHO launches mobile application to facilitate diagnosis. News release. World Health Organization; July 16, 2020. Accessed April 4, 2024. https://www.who.int/news/item/16-07-2020-neglected-tropical-diseases-of-the-skin-who-launches-mobile-application-to-facilitate-diagnosis<br/><br/>43. Padovese V, Fuller LC, Griffiths CEM, et al; Migrant Health Dermatology Working Group of the International Foundation for Dermatology. Migrant skin health: perspectives from the Migrant Health Summit, Malta, 2022. <i>Br J Dermatology</i>. 2023;188:553-554. doi:10.1093/bjd/ljad001 <br/><br/>44. Knapp AP, Rehmus W, Chang AY. Skin diseases in displaced populations: a review of contributing factors, challenges, and approaches to care. <i>Int J Dermato</i>l. 2020;59:1299-1311. doi:10.1111/ijd.15063<br/><br/>45. Norman FF, Comeche B, Chamorro S, et al. Overcoming challenges in the diagnosis and treatment of parasitic infectious diseases in migrants. <i>Expert Rev Anti-infective Therapy. </i>2020;18:127-143. doi:10.1080/14787210.2020.1713099<br/><br/>46. Skin NTDs: prioritizing integrated approaches to reduce suffering, psychosocial impact and stigmatization. News release. World Health Organization; October 29, 2020. Accessed April 4, 2024. https://www.who.int/news/item/29-10-2020-skin-ntds-prioritizing-integrated-approaches-to-reduce-suffering-psychosocial-impact-and-stigmatization</p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>bio</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> <p class="disclosure">Alexis G. Strahan is from the Mercer University School of Medicine, Savannah, Georgia. Dr. Elston is from the Department of Dermatology and Dermatologic Surgery, Medical University of South Carolina, Charleston.</p> <p class="disclosure">The authors report no conflict of interest. <br/><br/>All images are in the public domain. <br/><br/>Correspondence: Alexis G. Strahan, MD, MSN, 55 Fruit St, Bartlett Hall 6R, Boston, MA 02114 (<a href="mailto:alexis.grabow.strahan@live.mercer.edu">alexis.grabow.strahan@live.mercer.edu</a>). <br/><br/><em><hl name="17868"/>Cutis. </em>2024 April;113(4):E16-E21. doi:10.12788/cutis.0999 </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>in</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> <p class="insidehead">Practice <strong>Points</strong></p> <ul class="insidebody"> <li>War and natural disasters displace populations and disrupt infrastructure and access to medical care.</li> <li>Infestations and cutaneous infections are common among refugee populations, and impetigo often is a sign of underlying scabies infestation.</li> <li>Body lice are important disease vectors inrefugee populations. </li> </ul> </itemContent> </newsItem> </itemSet></root>
Practice Points
- War and natural disasters displace populations and disrupt infrastructure and access to medical care.
- Infestations and cutaneous infections are common among refugee populations, and impetigo often is a sign of underlying scabies infestation.
- Body lice are important disease vectors inrefugee populations.

Hepatitis Kills 3500 People Each Day, Says WHO
The number of deaths from viral hepatitis worldwide increased from 1.1 million in 2019 to 1.3 million in 2022. These figures equate to approximately 3500 deaths per day due to the disease, which is the second leading cause of mortality from infectious agents globally.
These data are part of the recently released Global Hepatitis Report 2024, which was published by the World Health Organization (WHO) during the World Hepatitis Summit in Lisbon, Portugal.
“This report paints a concerning picture: Despite global progress in preventing hepatitis infections, deaths are increasing because very few people with hepatitis are being diagnosed and treated,” said WHO Director-General Tedros Adhanom Ghebreyesus, PhD.
Hepatitis B significantly is associated with the highest mortality rate. It accounted for 83% of deaths from the disease in 2022. Meanwhile, hepatitis C was responsible for 17% of deaths. The mortality of other, less common types of hepatitis was not considered in the ranking.
The report also indicates that more than 6000 people worldwide are infected with viral hepatitis every day. The 2.2 million new cases in 2022 represent a slight decrease from 2.5 million in 2019, but the WHO considers the incidence high.
The organization’s updated statistics indicate that about 254 million people had hepatitis B in 2022, while 50 million had type C.
“Besides the deaths, the number of new cases every year is also striking. These are diseases that continue to spread. In the case of hepatitis C, the spread results from lack of access to disposable or properly sterilized sharp materials,” said Thor Dantas, MD, PhD, a physician and director of the Brazilian Society of Hepatology’s Viral Hepatitis Committee.
The situation of hepatitis B is particularly problematic, given that there is a safe and effective vaccine against it, said Dantas. “It’s remarkable that we continue to have so many new cases worldwide. This shows that we are failing in access to preventive measures for control and spread.”
Half of chronic hepatitis B and C cases occur in people between ages 30 and 54 years, while 12% affect children. There are more infections among men, who represent 58% of all cases.
The WHO also drew attention to the difficulty of accessing diagnosis and treatment. Only 13% of people with chronic hepatitis B infection were diagnosed, while only 3% — equivalent to 7 million people — received antiviral therapy by the end of 2022. This result is well below the WHO’s global target, which aims to treat 80% of cases by 2030.
Brazil has a higher diagnostic rate than the global average but is still below the target. According to the report, in 2022, the country diagnosed 34.2% of all hepatitis B infections. However, treatment coverage remains low: 3.6% of the total.
For hepatitis C, the scenario is somewhat different. During the same period, Brazil diagnosed 36% of total cases, with a treatment rate of 24%.
In 2022, Brazil had 2578 deaths from hepatitis B and 2977 from hepatitis C.
Because hepatitis is a silent disease, diagnosis often comes late, when the disease is already quite advanced, said Dr. Dantas. “Viral hepatitis evolves over the years essentially asymptomatically. Malaria shows symptoms, and tuberculosis shows symptoms. Viral hepatitis does not. They are only discovered through active searching.”
The WHO report shows significant regional differences in infection rates. Almost two thirds of cases are concentrated in the following 10 countries: China, India, Indonesia, Nigeria, Pakistan, Ethiopia, Bangladesh, Vietnam, the Philippines, and Russia.
In terms of hepatitis C incidence, Brazil ranks 15th globally, with 536,000 cases in 2022, representing 1.1% of the global total. The list is led by Pakistan, with 8.8 million cases, equivalent to 17.8% of the total. Next are India, with 5.5 million (11.2%), and China, with 4 million (8.1%).
In addition to regional differences, the report also reveals profound disparities in the prices paid for major treatments.
“Price disparities between, and even within, WHO regions persist, with many countries paying above global reference values, including for nonpatented medications,” according to the report.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
The number of deaths from viral hepatitis worldwide increased from 1.1 million in 2019 to 1.3 million in 2022. These figures equate to approximately 3500 deaths per day due to the disease, which is the second leading cause of mortality from infectious agents globally.
These data are part of the recently released Global Hepatitis Report 2024, which was published by the World Health Organization (WHO) during the World Hepatitis Summit in Lisbon, Portugal.
“This report paints a concerning picture: Despite global progress in preventing hepatitis infections, deaths are increasing because very few people with hepatitis are being diagnosed and treated,” said WHO Director-General Tedros Adhanom Ghebreyesus, PhD.
Hepatitis B significantly is associated with the highest mortality rate. It accounted for 83% of deaths from the disease in 2022. Meanwhile, hepatitis C was responsible for 17% of deaths. The mortality of other, less common types of hepatitis was not considered in the ranking.
The report also indicates that more than 6000 people worldwide are infected with viral hepatitis every day. The 2.2 million new cases in 2022 represent a slight decrease from 2.5 million in 2019, but the WHO considers the incidence high.
The organization’s updated statistics indicate that about 254 million people had hepatitis B in 2022, while 50 million had type C.
“Besides the deaths, the number of new cases every year is also striking. These are diseases that continue to spread. In the case of hepatitis C, the spread results from lack of access to disposable or properly sterilized sharp materials,” said Thor Dantas, MD, PhD, a physician and director of the Brazilian Society of Hepatology’s Viral Hepatitis Committee.
The situation of hepatitis B is particularly problematic, given that there is a safe and effective vaccine against it, said Dantas. “It’s remarkable that we continue to have so many new cases worldwide. This shows that we are failing in access to preventive measures for control and spread.”
Half of chronic hepatitis B and C cases occur in people between ages 30 and 54 years, while 12% affect children. There are more infections among men, who represent 58% of all cases.
The WHO also drew attention to the difficulty of accessing diagnosis and treatment. Only 13% of people with chronic hepatitis B infection were diagnosed, while only 3% — equivalent to 7 million people — received antiviral therapy by the end of 2022. This result is well below the WHO’s global target, which aims to treat 80% of cases by 2030.
Brazil has a higher diagnostic rate than the global average but is still below the target. According to the report, in 2022, the country diagnosed 34.2% of all hepatitis B infections. However, treatment coverage remains low: 3.6% of the total.
For hepatitis C, the scenario is somewhat different. During the same period, Brazil diagnosed 36% of total cases, with a treatment rate of 24%.
In 2022, Brazil had 2578 deaths from hepatitis B and 2977 from hepatitis C.
Because hepatitis is a silent disease, diagnosis often comes late, when the disease is already quite advanced, said Dr. Dantas. “Viral hepatitis evolves over the years essentially asymptomatically. Malaria shows symptoms, and tuberculosis shows symptoms. Viral hepatitis does not. They are only discovered through active searching.”
The WHO report shows significant regional differences in infection rates. Almost two thirds of cases are concentrated in the following 10 countries: China, India, Indonesia, Nigeria, Pakistan, Ethiopia, Bangladesh, Vietnam, the Philippines, and Russia.
In terms of hepatitis C incidence, Brazil ranks 15th globally, with 536,000 cases in 2022, representing 1.1% of the global total. The list is led by Pakistan, with 8.8 million cases, equivalent to 17.8% of the total. Next are India, with 5.5 million (11.2%), and China, with 4 million (8.1%).
In addition to regional differences, the report also reveals profound disparities in the prices paid for major treatments.
“Price disparities between, and even within, WHO regions persist, with many countries paying above global reference values, including for nonpatented medications,” according to the report.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
The number of deaths from viral hepatitis worldwide increased from 1.1 million in 2019 to 1.3 million in 2022. These figures equate to approximately 3500 deaths per day due to the disease, which is the second leading cause of mortality from infectious agents globally.
These data are part of the recently released Global Hepatitis Report 2024, which was published by the World Health Organization (WHO) during the World Hepatitis Summit in Lisbon, Portugal.
“This report paints a concerning picture: Despite global progress in preventing hepatitis infections, deaths are increasing because very few people with hepatitis are being diagnosed and treated,” said WHO Director-General Tedros Adhanom Ghebreyesus, PhD.
Hepatitis B significantly is associated with the highest mortality rate. It accounted for 83% of deaths from the disease in 2022. Meanwhile, hepatitis C was responsible for 17% of deaths. The mortality of other, less common types of hepatitis was not considered in the ranking.
The report also indicates that more than 6000 people worldwide are infected with viral hepatitis every day. The 2.2 million new cases in 2022 represent a slight decrease from 2.5 million in 2019, but the WHO considers the incidence high.
The organization’s updated statistics indicate that about 254 million people had hepatitis B in 2022, while 50 million had type C.
“Besides the deaths, the number of new cases every year is also striking. These are diseases that continue to spread. In the case of hepatitis C, the spread results from lack of access to disposable or properly sterilized sharp materials,” said Thor Dantas, MD, PhD, a physician and director of the Brazilian Society of Hepatology’s Viral Hepatitis Committee.
The situation of hepatitis B is particularly problematic, given that there is a safe and effective vaccine against it, said Dantas. “It’s remarkable that we continue to have so many new cases worldwide. This shows that we are failing in access to preventive measures for control and spread.”
Half of chronic hepatitis B and C cases occur in people between ages 30 and 54 years, while 12% affect children. There are more infections among men, who represent 58% of all cases.
The WHO also drew attention to the difficulty of accessing diagnosis and treatment. Only 13% of people with chronic hepatitis B infection were diagnosed, while only 3% — equivalent to 7 million people — received antiviral therapy by the end of 2022. This result is well below the WHO’s global target, which aims to treat 80% of cases by 2030.
Brazil has a higher diagnostic rate than the global average but is still below the target. According to the report, in 2022, the country diagnosed 34.2% of all hepatitis B infections. However, treatment coverage remains low: 3.6% of the total.
For hepatitis C, the scenario is somewhat different. During the same period, Brazil diagnosed 36% of total cases, with a treatment rate of 24%.
In 2022, Brazil had 2578 deaths from hepatitis B and 2977 from hepatitis C.
Because hepatitis is a silent disease, diagnosis often comes late, when the disease is already quite advanced, said Dr. Dantas. “Viral hepatitis evolves over the years essentially asymptomatically. Malaria shows symptoms, and tuberculosis shows symptoms. Viral hepatitis does not. They are only discovered through active searching.”
The WHO report shows significant regional differences in infection rates. Almost two thirds of cases are concentrated in the following 10 countries: China, India, Indonesia, Nigeria, Pakistan, Ethiopia, Bangladesh, Vietnam, the Philippines, and Russia.
In terms of hepatitis C incidence, Brazil ranks 15th globally, with 536,000 cases in 2022, representing 1.1% of the global total. The list is led by Pakistan, with 8.8 million cases, equivalent to 17.8% of the total. Next are India, with 5.5 million (11.2%), and China, with 4 million (8.1%).
In addition to regional differences, the report also reveals profound disparities in the prices paid for major treatments.
“Price disparities between, and even within, WHO regions persist, with many countries paying above global reference values, including for nonpatented medications,” according to the report.
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167849</fileName> <TBEID>0C04FCC5.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FCC5</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240424T164356</QCDate> <firstPublished>20240424T164404</firstPublished> <LastPublished>20240424T164404</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240424T164404</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Giuliana Miranda</byline> <bylineText>GIULIANA MIRANDA</bylineText> <bylineFull>GIULIANA MIRANDA</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType>News</newsDocType> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>The report reveals that despite advances in diagnostic tools and treatment options, global treatment rates and coverage for detection tests have stagnated.</metaDescription> <articlePDF/> <teaserImage/> <teaser>WHO’s World Hepatitis Summit finds that diagnosis and treatments have improved, yet testing and utilized therapies have stalled.</teaser> <title>Hepatitis Kills 3500 People Each Day, Says WHO</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term canonical="true">20</term> <term>21</term> <term>15</term> </publications> <sections> <term canonical="true">39313</term> </sections> <topics> <term canonical="true">314</term> <term>234</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Hepatitis Kills 3500 People Each Day, Says WHO</title> <deck/> </itemMeta> <itemContent> <p><br/><br/>The number of deaths from <span class="Hyperlink">viral hepatitis</span> worldwide increased from 1.1 million in 2019 to 1.3 million in 2022. These figures equate to approximately 3500 deaths per day due to the disease, which is the second leading cause of mortality from infectious agents globally.<br/><br/>These data are part of the recently released <span class="Hyperlink"><a href="https://www.who.int/publications/i/item/9789240091672">Global Hepatitis Report 2024</a></span>, which was published by the World Health Organization (WHO) during the World Hepatitis Summit in Lisbon, Portugal.<br/><br/><span class="tag metaDescription">The report reveals that despite advances in diagnostic tools and treatment options, global treatment rates and coverage for detection tests have stagnated.</span><br/><br/>“This report paints a concerning picture: Despite global progress in preventing hepatitis infections, deaths are increasing because very few people with hepatitis are being diagnosed and treated,” said WHO Director-General Tedros Adhanom Ghebreyesus, PhD.<br/><br/><span class="Hyperlink">Hepatitis B</span> significantly is associated with the highest mortality rate. It accounted for 83% of deaths from the disease in 2022. Meanwhile, <span class="Hyperlink">hepatitis C</span> was responsible for 17% of deaths. The mortality of other, less common types of hepatitis was not considered in the ranking.<br/><br/>The report also indicates that more than 6000 people worldwide are infected with viral hepatitis every day. The 2.2 million new cases in 2022 represent a slight decrease from 2.5 million in 2019, but the WHO considers the incidence high.<br/><br/>The organization’s updated statistics indicate that about 254 million people had hepatitis B in 2022, while 50 million had type C.<br/><br/>“Besides the deaths, the number of new cases every year is also striking. These are diseases that continue to spread. In the case of hepatitis C, the spread results from lack of access to disposable or properly sterilized sharp materials,” said Thor Dantas, MD, PhD, a physician and director of the Brazilian Society of Hepatology’s Viral Hepatitis Committee.<br/><br/>The situation of hepatitis B is particularly problematic, given that there is a safe and effective vaccine against it, said Dantas. “It’s remarkable that we continue to have so many new cases worldwide. This shows that we are failing in access to preventive measures for control and spread.”<br/><br/>Half of chronic hepatitis B and C cases occur in people between ages 30 and 54 years, while 12% affect children. There are more infections among men, who represent 58% of all cases.<br/><br/>The WHO also drew attention to the difficulty of accessing diagnosis and treatment. Only 13% of people with chronic hepatitis B infection were diagnosed, while only 3% — equivalent to 7 million people — received antiviral therapy by the end of 2022. This result is well below the WHO’s global target, which aims to treat 80% of cases by 2030.<br/><br/>Brazil has a higher diagnostic rate than the global average but is still below the target. According to the report, in 2022, the country diagnosed 34.2% of all hepatitis B infections. However, treatment coverage remains low: 3.6% of the total.<br/><br/>For hepatitis C, the scenario is somewhat different. During the same period, Brazil diagnosed 36% of total cases, with a treatment rate of 24%.<br/><br/>In 2022, Brazil had 2578 deaths from hepatitis B and 2977 from hepatitis C.<br/><br/>Because hepatitis is a silent disease, diagnosis often comes late, when the disease is already quite advanced, said Dr. Dantas. “Viral hepatitis evolves over the years essentially asymptomatically. <span class="Hyperlink">Malaria</span> shows symptoms, and <span class="Hyperlink">tuberculosis</span> shows symptoms. Viral hepatitis does not. They are only discovered through active searching.”<br/><br/>The WHO report shows significant regional differences in infection rates. Almost two thirds of cases are concentrated in the following 10 countries: China, India, Indonesia, Nigeria, Pakistan, Ethiopia, Bangladesh, Vietnam, the Philippines, and Russia.<br/><br/>In terms of hepatitis C incidence, Brazil ranks 15th globally, with 536,000 cases in 2022, representing 1.1% of the global total. The list is led by Pakistan, with 8.8 million cases, equivalent to 17.8% of the total. Next are India, with 5.5 million (11.2%), and China, with 4 million (8.1%).<br/><br/>In addition to regional differences, the report also reveals profound disparities in the prices paid for major treatments.<br/><br/>“Price disparities between, and even within, WHO regions persist, with many countries paying above global reference values, including for nonpatented medications,” according to the report.<br/><br/></p> <p> <em>This story was translated from the <span class="Hyperlink"><a href="https://portugues.medscape.com/verartigo/6510952">Medscape Portuguese</a></span> edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication.A version of this article appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/hepatitis-kills-3-5-million-people-each-day-says-who-2024a10007xi?src=">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
Syphilis Treatment Falls Short for Pregnant Patients
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.
Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.
To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.
The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The findings were published in Obstetrics & Gynecology.
Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.
Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).
The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.
The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.
More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.
The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167766</fileName> <TBEID>0C04FABE.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FABE</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname>syphilis4.17.24</storyname> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240424T121054</QCDate> <firstPublished>20240424T123826</firstPublished> <LastPublished>20240424T123826</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240424T123826</CMSDate> <articleSource>FROM OBSTETRICS & GYNECOLOGY</articleSource> <facebookInfo/> <meetingNumber/> <byline>Heidi Splete</byline> <bylineText>HEIDI SPLETE</bylineText> <bylineFull>HEIDI SPLETE</bylineFull> <bylineTitleText>MDedge News</bylineTitleText> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, base</metaDescription> <articlePDF/> <teaserImage/> <teaser>Potential challenges to effective treatment of syphilis in pregnancy include drug shortages and time constraints.</teaser> <title>Syphilis Treatment Falls Short for Pregnant Patients</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>ob</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term>15</term> <term canonical="true">20</term> <term>23</term> </publications> <sections> <term>27970</term> <term canonical="true">39313</term> </sections> <topics> <term>234</term> <term>322</term> <term>280</term> <term>271</term> <term canonical="true">50729</term> <term>294</term> <term>71135</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Syphilis Treatment Falls Short for Pregnant Patients</title> <deck/> </itemMeta> <itemContent> <p>Approximately one third of pregnant individuals with syphilis were inadequately treated or not treated for syphilis despite receiving timely prenatal care, based on data from nearly 1500 patients.</p> <p>Although congenital syphilis is preventable with treatment before or early in pregnancy, data from the Centers for Disease Control and Prevention (CDC) show a doubling of syphilis rates in the United States between 2018 and 2021 wrote Ayzsa Tannis, MPH, of the Centers for Disease Control and Prevention, Atlanta, and colleagues.<br/><br/>To better understand factors contributing to inadequate syphilis treatment during pregnancy, the researchers examined data from 1476 individuals with syphilis during pregnancy. The study population came from six jurisdictions that participated in the Surveillance for Emerging Threats to Pregnant People and Infants Network, and sources included case investigations, medical records, and links between laboratory data and vital records.<br/><br/>The researchers characterized the status of syphilis during pregnancy as adequate, inadequate, or not treated based on the CDC’s Sexually Transmitted Infections Treatment Guidelines, 2021. Prenatal care was defined as timely (at least 30 days prior to pregnancy outcome), nontimely (less than 30 days before pregnancy outcome), and no prenatal care. The <span class="Hyperlink">findings</span> <span class="Hyperlink"><a href="https://journals.lww.com/greenjournal/abstract/9900/syphilis_treatment_among_people_who_are_pregnant.1059.aspx">were published</a></span> in <em>Obstetrics & Gynecology</em>. <br/><br/>Of the 1476 individuals studied, 855 (57.9%) were adequately treated for syphilis and 621 (42.1%) were inadequately or not treated.<br/><br/>Overall, 82% of the study population received timely prenatal care. However, 32.1% of those who received timely prenatal care were inadequately treated, including 14.8% who received no syphilis treatment. Individuals with nontimely or no prenatal care were significantly more likely to receive inadequate or no treatment for syphilis than those who received timely care (risk ratio, 2.50 and 2.73, respectively).<br/><br/>The findings were consistent with previous studies of missed opportunities for prevention and treatment, the researchers noted. Factors behind nontimely treatment (less than 30 days before pregnancy outcome) may include intermittent shortages of benzathine penicillin G, the standard treatment for syphilis, as well as the lack of time and administrative support for clinicians to communicate with patients and health departments, and to expedite treatment, the researchers wrote.<br/><br/>The results were limited by several factors including the use of data from six US jurisdictions that may not generalize to other areas, the variations in reporting years for the different jurisdictions, and variation in mandates for syphilis screening during pregnancy, the researchers noted.<br/><br/>More research is needed to improve syphilis testing itself, and to develop more treatment options, the researchers concluded. Partnerships among public health, patient advocacy groups, prenatal care clinicians, and other clinicians outside the prenatal care setting also are needed for effective intervention in pregnant individuals with syphilis, they said.<br/><br/>The study was carried out as part of the regular work of the CDC, supported by the Epidemiology and Laboratory Capacity for Prevention and Control of Emerging Infectious Diseases Cooperative Agreement and through contractual mechanisms including the Local Health Department Initiative to Chickasaw Health Consulting. The researchers had no financial conflicts to disclose.<span class="end"/></p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
FROM OBSTETRICS & GYNECOLOGY
Menopause, RSV, and More: 4 New Meds to Know
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
BOSTON — The US Food and Drug Administration (FDA) approved 55 new medications in 2023 and 11 more in 2024 to date.
A New First-Line for GERD?
Vonoprazan, an oral potassium-competitive acid blocker — which received FDA approval in November 2023 — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat gastroesophageal reflux disease (GERD).
GERD is the most common gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.
“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees.
Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.
The approval of vonoprazan for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than lansoprazole in treating erosive esophagitis.
Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.
Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.
Nonhormonal Drug for Menopause
Fezolinetant, the first neurokinin receptor antagonist to receive approval from the FDA to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.
“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.
Results from the SKYLIGHT 1 randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, diarrhea, and insomnia.
Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), gabapentin, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the North American Menopause Society.
“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”
RSV Vaccine for Everyone
Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US Centers for Disease Control and Prevention.
The FDA has approved two RSV vaccines approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.
Patients who received the RSV vaccine had an 83% relative risk reduction for the illness, according to a recent study, and an overall lower risk for hospitalization.
Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines. A study published in 2023 in The New England Journal of Medicine found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.
“This is important given ongoing concerns of neurological safety,” among older adults who receive the RSV vaccine, Dr. Smetana said.
As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s Adult RSV Work Group plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.
New Antidepressants
A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.
Gepirone, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression.
Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. In 2015, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.
“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.”
Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said.
Studies suggest that gepirone reduces both anxiety and depression scores on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of depression relapse compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause sexual dysfunction in men, Dr. Smetana said.
Gepirone will be available to prescribe to patients in fall 2024.
Dr. Smetana reported no relevant financial conflicts of interest.
A version of this article appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167807</fileName> <TBEID>0C04FBBF.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FBBF</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240423T110410</QCDate> <firstPublished>20240423T114823</firstPublished> <LastPublished>20240423T114823</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240423T114823</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Lara Salahi</byline> <bylineText>LARA SALAHI</bylineText> <bylineFull>LARA SALAHI</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType>News</newsDocType> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>During a presentation on April 18 at the annual American College of Physicians Internal Medicine Meeting, Gerald Smetana, MD, professor of medicine in the Divis</metaDescription> <articlePDF/> <teaserImage/> <teaser>New treatments have been approved to treat conditions including GERD, depression, RSV vaccines, and hot flashes with menopause.</teaser> <title>Menopause, RSV, and More: 4 New Meds to Know</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>ob</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>chph</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>cpn</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term canonical="true">21</term> <term>23</term> <term>15</term> <term>20</term> <term>6</term> <term>9</term> </publications> <sections> <term canonical="true">39313</term> </sections> <topics> <term>202</term> <term canonical="true">65668</term> <term>322</term> <term>247</term> <term>234</term> <term>248</term> <term>50347</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Menopause, RSV, and More: 4 New Meds to Know</title> <deck/> </itemMeta> <itemContent> <p><span class="dateline">BOSTON</span> — The US Food and Drug Administration (FDA) approved <span class="Hyperlink">55 new medications</span> in 2023 and <span class="Hyperlink"><a href="https://www.fda.gov/drugs/novel-drug-approvals-fda/novel-drug-approvals-2024">11 more in 2024 to date</a></span>. <span class="tag metaDescription">During a presentation on April 18 at the annual American College of Physicians Internal Medicine Meeting, Gerald Smetana, MD, professor of medicine in the Division of General Medicine at Beth Israel Deaconess Medical Center in Boston, reviewed four of these new therapies that are likely to be particularly important for primary care clinicians. </span></p> <h2>A New First-Line for GERD?</h2> <p>Vonoprazan, an oral potassium-competitive acid blocker — which received<span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/998031"> FDA approval in November 2023</a></span> — may be a good alternative for patients whose symptoms continue to linger despite taking medications designated to treat <span class="Hyperlink">gastroesophageal reflux disease</span> (GERD). <br/><br/>GERD is the<span class="Hyperlink"><a href="https://pubmed.ncbi.nlm.nih.gov/30323268/"> most common</a></span> gastrointestinal symptom encountered by primary care physicians. Proton-pump inhibitors (PPIs) are the first-line treatment for the condition but can have long-term side effects such as Clostridioides difficile infection and kidney lesions.<br/><br/>“We know that not all patients are going to have symptom relief with H2 blockers and PPIs, so there’s an opportunity for patients who don’t get full symptom relief,” Dr. Smetana told attendees. <br/><br/>Vonoprazan blocks potassium binding to ATPase proton pumps and inhibits the secretion of gastric acid.<br/><br/>The <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/998031">approval of vonoprazan</a></span> for erosive GERD was based on results from the phase 3 PHALCON-EE study, a randomized, double-blind, multicenter study that found the drug to be more effective than <span class="Hyperlink"><a href="https://reference.medscape.com/drug/prevacid-solu-tab-lansoprazole-341991">lansoprazole</a></span> in treating erosive <span class="Hyperlink">esophagitis</span>.<br/><br/>Vonoprazan “has more rapid absorption than PPIs [and a] longer half-life and is more potent than PPIs, so theoretically it could be more effective in certain settings,” Dr. Smetana said.<br/><br/>Vonoprazan is FDA approved for only 6 months of use. Despite its efficacy, cost may be a barrier to many patients. H2 blockers generally cost patients less than $10 for 1 month’s supply, whereas vonoprazan can cost up to $650.<br/><br/></p> <h2>Nonhormonal Drug for Menopause</h2> <p><span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/992670">Fezolinetant</a></span>, the first neurokinin receptor antagonist to receive <span class="Hyperlink"><a href="https://www.fda.gov/news-events/press-announcements/fda-approves-novel-drug-treat-moderate-severe-hot-flashes-caused-menopause">approval from the FDA</a></span> to treat vasomotor symptoms, may be an option for women concerned about hormone-based therapy for menopausal hot flashes.<br/><br/>“[Fezolinetant] specifically works in the area of the brain that’s involved in body temperature regulation and sweating,” Dr. Smetana said.<br/><br/>Results from the<span class="Hyperlink"><a href="https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)00085-5/abstract"> SKYLIGHT 1</a></span> randomized controlled trial of fezolinetant found the medication reduced the frequency and severity of hot flashes. Some of the side effects include abdominal pain, <span class="Hyperlink">diarrhea</span>, and <span class="Hyperlink">insomnia</span>. <br/><br/>Other nonestrogen treatments, including selective serotonin reuptake inhibitors (SSRIs), <span class="Hyperlink">gabapentin</span>, cognitive-behavioral therapy, and hypnosis, are modestly effective, according to the<span class="Hyperlink"><a href="https://www.menopause.org/for-women/menopause-faqs-hot-flashes"> North American Menopause Society</a></span>.<br/><br/>“[Fezolinetant] offers a different option that physicians may be more comfortable prescribing,” Dr. Smetana said. “And I think this will be an important addition to nonhormonal therapy.”<br/><br/></p> <h2>RSV Vaccine for Everyone </h2> <p>Once considered an illness that is more prevalent in young children, respiratory syncytial virus (RSV) has become more prevalent and severe among older adults. Between 60,000 and 120,000 older adults are hospitalized and 6000-10,000 die of RSV infection each year, according to the US<span class="Hyperlink"><a href="https://www.cdc.gov/rsv/high-risk/older-adults.html"> Centers for Disease Control and Prevention</a></span>. <br/><br/>The FDA has approved<span class="Hyperlink"> two RSV vaccines</span> approved for older adults, but clinicians may find it challenging to get older patients vaccinated for this and other preventable illnesses.<br/><br/>Patients who received the <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/994631">RSV vaccine</a></span> had an 83% relative risk reduction for the illness,<span class="Hyperlink"><a href="https://pubmed.ncbi.nlm.nih.gov/36791160/"> according to a recent study</a></span>, and an overall lower risk for hospitalization.<br/><br/>Moderna is developing an mRNA vaccine for RSV that is similar to many COVID-19 vaccines.<span class="Hyperlink"> <a href="https://www.nejm.org/doi/full/10.1056/NEJMoa2307079">A study</a> published in 2023 in </span><em>The New England Journal of Medicine </em>found no cases of neuroinflammatory disorders among patients who received the mRNA RSV vaccine, with a median follow-up of 112 days.<br/><br/>“This is important given ongoing concerns of<span class="Hyperlink"> neurological safety</span>,” among older adults who receive the RSV vaccine, Dr. Smetana said.<br/><br/>As of March 2024, the CDC recommends shared decision-making for adults older than 60 years and for healthcare providers to “consider” rather than “recommend” the vaccine for their patients. The agency’s<span class="Hyperlink"><a href="https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2024-02-28-29/08-RSV-Adults-Britton-508.pdf"> Adult RSV Work Group</a></span> plans to meet at June 2024 to reconsider whether shared clinical decision-making remains the preferred policy option.<br/><br/></p> <h2>New Antidepressants</h2> <p>A medication thrice rejected by the FDA is now heading a new class of drugs to treat major depressive disorder.<br/><br/><span class="Hyperlink"><a href="https://reference.medscape.com/drug/exxua-gepirone-1000091">Gepirone</a></span>, a 5-HT1A receptor agonist, has a different mechanism of action from that of SSRIs, which are currently considered the first-line treatment for depression. <br/><br/>Gepirone was rejected by the FDA in 2002, 2004, and 2007, with concerns that the efficacy studies were too small. <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/855373">In 2015</a></span>, an FDA advisory committee agreed that the evidence to date did not support approval of an extended-release form of the drug. But the agency decided to approve the medication in September 2023.<br/><br/>“So why is this medication worth discussing now?” Dr. Smetana said. “It’s because the side effect profile is different from existing antidepressants.” <br/><br/>Many patients may stop using SSRIs because of side effects such as insomnia and loss of libido, Dr. Smetana said. Gepirone has the potential to avoid activation of other 5-HT receptors that mediate side effects, he said. <br/><br/>Studies suggest that gepirone <span class="Hyperlink"><a href="https://pubmed.ncbi.nlm.nih.gov/11206598/">reduces both anxiety and depression scores</a></span> on the Hamilton Depression Rating Scale in patients who have both conditions and decreases rates of<span class="Hyperlink"><a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2943802/"> depression relapse</a></span> compared with placebo through at least 48 weeks. The drug also may be less likely than SSRIs to cause<span class="Hyperlink"><a href="https://onlinelibrary.wiley.com/doi/abs/10.1111/j.1743-6109.2011.02624.x"> sexual dysfunction</a></span> in men, Dr. Smetana said. <br/><br/>Gepirone will be available to prescribe to patients in <span class="Hyperlink">fall 2024.<br/><br/></span>Dr. Smetana reported no relevant financial conflicts of interest.<span class="end"/> <br/><br/></p> <p> <em>A version of this article appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/menopause-rsv-and-more-4-new-meds-know-2024a10007m3">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
Ocular Microbiome May Be Dry Eye Culprit
A mix of microbes may help explain why some people develop dry eye disease, new research showed.
This finding suggests that bacteria may cause dry eye and could someday point to new treatments for the condition and related disorders, which affect an estimated 27 million Americans, according to researchers.
Current treatments aim to preserve and enhance tears and tear production to ease the grittiness and itchiness that accompany dry eye disease.
To examine the role of the ocular microbiome in dry eye disease, scientists in Texas analyzed swab samples from 30 men and women, nine of whom had dry eye.
They found Streptococcus and Pedobacter species were the most common bacteria in healthy eyes.
In people with dry eye, however, more Acinetobacter species were detected.
“We think the metabolites produced by these bacteria are responsible for dry eye conditions,” study coauthor Pallavi Sharma said in a news release about the findings.
Sharma, a graduate student at Stephen F. Austin State University in Nacogdoches, Texas, presented this research last month at the annual meeting of the American Society for Biochemistry and Molecular Biology. The research team was led by Alexandra Van Kley, PhD, a professor of biology at the university.
“Once we understand the eye microbiota properly, it will improve disease diagnosis at an early stage,” Van Kley predicted in the news release. “This knowledge can also serve as a catalyst for developing innovative therapies aimed at preventing and treating ocular disease as well as those that affect the central microbiome site: The gut.”
Investigators in Australia have conducted similar experiments in patients with meibomian gland dysfunction, a condition marked by underproduction of key oils in the eye.
One group reported in August 2023 the finding of “detectable differences in the bacterial richness, diversity, and community structure of the conjunctiva and eyelid margin between individuals with meibomian gland dysfunction with and without lacrimal dysfunction, as well as to healthy controls.”
More research is needed to confirm and understand the findings, though, and “to determine if manipulating the microbiome could be a potential treatment for the condition,” they wrote.
A version of this article appeared on Medscape.com.
A mix of microbes may help explain why some people develop dry eye disease, new research showed.
This finding suggests that bacteria may cause dry eye and could someday point to new treatments for the condition and related disorders, which affect an estimated 27 million Americans, according to researchers.
Current treatments aim to preserve and enhance tears and tear production to ease the grittiness and itchiness that accompany dry eye disease.
To examine the role of the ocular microbiome in dry eye disease, scientists in Texas analyzed swab samples from 30 men and women, nine of whom had dry eye.
They found Streptococcus and Pedobacter species were the most common bacteria in healthy eyes.
In people with dry eye, however, more Acinetobacter species were detected.
“We think the metabolites produced by these bacteria are responsible for dry eye conditions,” study coauthor Pallavi Sharma said in a news release about the findings.
Sharma, a graduate student at Stephen F. Austin State University in Nacogdoches, Texas, presented this research last month at the annual meeting of the American Society for Biochemistry and Molecular Biology. The research team was led by Alexandra Van Kley, PhD, a professor of biology at the university.
“Once we understand the eye microbiota properly, it will improve disease diagnosis at an early stage,” Van Kley predicted in the news release. “This knowledge can also serve as a catalyst for developing innovative therapies aimed at preventing and treating ocular disease as well as those that affect the central microbiome site: The gut.”
Investigators in Australia have conducted similar experiments in patients with meibomian gland dysfunction, a condition marked by underproduction of key oils in the eye.
One group reported in August 2023 the finding of “detectable differences in the bacterial richness, diversity, and community structure of the conjunctiva and eyelid margin between individuals with meibomian gland dysfunction with and without lacrimal dysfunction, as well as to healthy controls.”
More research is needed to confirm and understand the findings, though, and “to determine if manipulating the microbiome could be a potential treatment for the condition,” they wrote.
A version of this article appeared on Medscape.com.
A mix of microbes may help explain why some people develop dry eye disease, new research showed.
This finding suggests that bacteria may cause dry eye and could someday point to new treatments for the condition and related disorders, which affect an estimated 27 million Americans, according to researchers.
Current treatments aim to preserve and enhance tears and tear production to ease the grittiness and itchiness that accompany dry eye disease.
To examine the role of the ocular microbiome in dry eye disease, scientists in Texas analyzed swab samples from 30 men and women, nine of whom had dry eye.
They found Streptococcus and Pedobacter species were the most common bacteria in healthy eyes.
In people with dry eye, however, more Acinetobacter species were detected.
“We think the metabolites produced by these bacteria are responsible for dry eye conditions,” study coauthor Pallavi Sharma said in a news release about the findings.
Sharma, a graduate student at Stephen F. Austin State University in Nacogdoches, Texas, presented this research last month at the annual meeting of the American Society for Biochemistry and Molecular Biology. The research team was led by Alexandra Van Kley, PhD, a professor of biology at the university.
“Once we understand the eye microbiota properly, it will improve disease diagnosis at an early stage,” Van Kley predicted in the news release. “This knowledge can also serve as a catalyst for developing innovative therapies aimed at preventing and treating ocular disease as well as those that affect the central microbiome site: The gut.”
Investigators in Australia have conducted similar experiments in patients with meibomian gland dysfunction, a condition marked by underproduction of key oils in the eye.
One group reported in August 2023 the finding of “detectable differences in the bacterial richness, diversity, and community structure of the conjunctiva and eyelid margin between individuals with meibomian gland dysfunction with and without lacrimal dysfunction, as well as to healthy controls.”
More research is needed to confirm and understand the findings, though, and “to determine if manipulating the microbiome could be a potential treatment for the condition,” they wrote.
A version of this article appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167773</fileName> <TBEID>0C04FB03.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FB03</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240419T105317</QCDate> <firstPublished>20240419T110344</firstPublished> <LastPublished>20240419T110344</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240419T110344</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Jake Remaly</byline> <bylineText>JAKE REMALY</bylineText> <bylineFull>JAKE REMALY</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>A mix of microbes may help explain why some people develop dry eye disease, new research showed.</metaDescription> <articlePDF/> <teaserImage/> <teaser>Study authors propose that the metabolites of <em>Acinetobacter</em> species, which are more common in dry eyes, contribute to the condition.</teaser> <title>Ocular Microbiome May Be Dry Eye Culprit</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term>15</term> <term canonical="true">21</term> </publications> <sections> <term>27970</term> <term canonical="true">39313</term> </sections> <topics> <term canonical="true">231</term> <term>234</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Ocular Microbiome May Be Dry Eye Culprit</title> <deck/> </itemMeta> <itemContent> <p>A mix of microbes may help explain why some people develop <span class="Hyperlink"><a href="https://emedicine.medscape.com/article/1210417-overview">dry eye</a></span> disease, new research showed.</p> <p>This finding suggests that bacteria may cause dry eye and could someday point to new treatments for the condition and related disorders, which affect <span class="Hyperlink"><a href="https://jamanetwork.com/journals/jamaophthalmology/fullarticle/2797832">an estimated</a></span> 27 million Americans, according to researchers.<br/><br/>Current treatments aim to preserve and enhance tears and tear production to ease the grittiness and itchiness that accompany dry eye disease. <br/><br/>To examine the role of the ocular microbiome in dry eye disease, scientists in Texas analyzed swab samples from 30 men and women, nine of whom had dry eye.<br/><br/>They found <em>Streptococcus</em> and <em>Pedobacter</em> species were the most common bacteria in healthy eyes.<br/><br/>In people with dry eye, however, more <em>Acinetobacter</em> species were detected.<br/><br/>“We think the metabolites produced by these bacteria are responsible for dry eye conditions,” study coauthor Pallavi Sharma <span class="Hyperlink"><a href="https://www.eurekalert.org/news-releases/1037703">said in a news release</a></span> about the findings. <br/><br/>Sharma, a graduate student at Stephen F. Austin State University in Nacogdoches, Texas, presented this research last month at the annual meeting of the American Society for Biochemistry and Molecular Biology. The research team was led by Alexandra Van Kley, PhD, a professor of biology at the university.<br/><br/>“Once we understand the eye microbiota properly, it will improve disease diagnosis at an early stage,” Van Kley predicted in the news release. “This knowledge can also serve as a catalyst for developing innovative therapies aimed at preventing and treating ocular disease as well as those that affect the central microbiome site: The gut.”<br/><br/>Investigators in Australia have conducted similar experiments in patients with meibomian gland dysfunction, a condition marked by underproduction of key oils in the eye.<br/><br/>One group <span class="Hyperlink"><a href="https://www.sciencedirect.com/science/article/pii/S0014483523002361?via%3Dihub">reported in August 2023</a></span> the finding of “detectable differences in the bacterial richness, diversity, and community structure of the conjunctiva and eyelid margin between individuals with meibomian gland dysfunction with and without lacrimal dysfunction, as well as to healthy controls.”<br/><br/>More research is needed to confirm and understand the findings, though, and “to determine if manipulating the microbiome could be a potential treatment for the condition,” they wrote.</p> <p> <em>A version of this article appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/ocular-microbiome-may-be-dry-eye-culprit-2024a10007go">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
Vaccine ‘Will Not Curb’ Dengue Epidemic, Says PAHO
The current tetravalent dengue vaccine TAK-003, from the Japanese laboratory Takeda, is not likely to control the ongoing epidemic, according to the Pan American Health Organization (PAHO). The organization emphasized the need to better understand the vaccine’s effectiveness against different serotypes and its safety under real-world clinical conditions.
The Americas are experiencing a record increase in dengue cases. Three times as many cases have been identified during 2024 (3.5 million) than were reported for the same period in 2023.
“The vaccine we have available will not curb the dengue epidemic; it should be used complementarily with other actions. The most important actions are field operations, vector control, prevention, and education,” said Daniel Salas, MD, executive manager of the PAHO Comprehensive Immunization Program, during a press conference on March 28.
“The vaccines we currently have are not the best response to reduce transmission and prevent deaths,” added Jarbas Barbosa, MD, PhD, PAHO’s director. The fatality rate remains below 0.05%, but this figure could be hard to maintain if the situation becomes more uncontrolled.
The TAK-003 regimen consists of two doses with a 3-month interval between applications, so “it is not a tool to control transmission at this moment. Studies have shown that only 8 years of [population-level] vaccination would have a significant impact on dengue transmission,” said Dr. Barbosa.
A new vaccine developed in Brazil in partnership with the company MSD, Butantan-DV, is in phase 3 trials and has the advantage of being a single-dose application, which could facilitate its use in situations with accelerated transmission. “But this vaccine will likely only be available in 2025,” said Dr. Barbosa.
PAHO officials also highlighted the need to better characterize the vaccine’s effectiveness and safety in the real world. They observed, for example, that when TAK-003 was investigated, the circulation of dengue serotype 3 was almost nonexistent, so the efficacy data against that serotype “are very limited.”
“The producer, Takeda, has very limited production capacity. Brazil is the country that uses this vaccine the most, followed by Argentina. Given that these countries have a good epidemiological surveillance system and adverse effect registration, they can conduct studies on how the vaccine performs in real life, which will greatly increase our knowledge about it. For example, we will see its effectiveness against serotype 3,” said Dr. Barbosa.
The PAHO Technical Advisory Group (TAG) on vaccine-preventable diseases recommended that any country using these vaccines have surveillance systems in place because it is important to promptly report and investigate any adverse events, said Dr. Salas. The organization also suggested that vaccination should ideally be administered in a “more controlled environment,” a phase 4 study, “to complete the safety and efficacy profile, especially in those who have not had dengue before and for dengue 3 and 4,” said Dr. Salas in response to a question from this news organization.
“People cannot expect that just because they were vaccinated, they will not get dengue. The vaccine has limited reach,” he emphasized.
Other research strategies for vector control, such as the use of the Wolbachia bacteria and mosquito sterilization, are future strategies and “not tools to control this outbreak,” noted Sylvain Aldighieri, MD, director of the Department of Prevention, Control, and Elimination of Transmissible Diseases at PAHO.
In his opening remarks, Dr. Barbosa urged the intensification of efforts with tools that are already available. These approaches include eliminating mosquito breeding sites (“80% are in or near homes”) and protecting against mosquito bites, preparing health services for early diagnosis and timely clinical management, and educating the population about dengue symptoms so they seek medical attention immediately.
Although dengue is increasing throughout Latin America and the Caribbean, the most affected countries are Brazil (83%), Paraguay (5.3%), and Argentina (3.7%), which account for 92% of the cases and 87% of the deaths, PAHO reported.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com .
The current tetravalent dengue vaccine TAK-003, from the Japanese laboratory Takeda, is not likely to control the ongoing epidemic, according to the Pan American Health Organization (PAHO). The organization emphasized the need to better understand the vaccine’s effectiveness against different serotypes and its safety under real-world clinical conditions.
The Americas are experiencing a record increase in dengue cases. Three times as many cases have been identified during 2024 (3.5 million) than were reported for the same period in 2023.
“The vaccine we have available will not curb the dengue epidemic; it should be used complementarily with other actions. The most important actions are field operations, vector control, prevention, and education,” said Daniel Salas, MD, executive manager of the PAHO Comprehensive Immunization Program, during a press conference on March 28.
“The vaccines we currently have are not the best response to reduce transmission and prevent deaths,” added Jarbas Barbosa, MD, PhD, PAHO’s director. The fatality rate remains below 0.05%, but this figure could be hard to maintain if the situation becomes more uncontrolled.
The TAK-003 regimen consists of two doses with a 3-month interval between applications, so “it is not a tool to control transmission at this moment. Studies have shown that only 8 years of [population-level] vaccination would have a significant impact on dengue transmission,” said Dr. Barbosa.
A new vaccine developed in Brazil in partnership with the company MSD, Butantan-DV, is in phase 3 trials and has the advantage of being a single-dose application, which could facilitate its use in situations with accelerated transmission. “But this vaccine will likely only be available in 2025,” said Dr. Barbosa.
PAHO officials also highlighted the need to better characterize the vaccine’s effectiveness and safety in the real world. They observed, for example, that when TAK-003 was investigated, the circulation of dengue serotype 3 was almost nonexistent, so the efficacy data against that serotype “are very limited.”
“The producer, Takeda, has very limited production capacity. Brazil is the country that uses this vaccine the most, followed by Argentina. Given that these countries have a good epidemiological surveillance system and adverse effect registration, they can conduct studies on how the vaccine performs in real life, which will greatly increase our knowledge about it. For example, we will see its effectiveness against serotype 3,” said Dr. Barbosa.
The PAHO Technical Advisory Group (TAG) on vaccine-preventable diseases recommended that any country using these vaccines have surveillance systems in place because it is important to promptly report and investigate any adverse events, said Dr. Salas. The organization also suggested that vaccination should ideally be administered in a “more controlled environment,” a phase 4 study, “to complete the safety and efficacy profile, especially in those who have not had dengue before and for dengue 3 and 4,” said Dr. Salas in response to a question from this news organization.
“People cannot expect that just because they were vaccinated, they will not get dengue. The vaccine has limited reach,” he emphasized.
Other research strategies for vector control, such as the use of the Wolbachia bacteria and mosquito sterilization, are future strategies and “not tools to control this outbreak,” noted Sylvain Aldighieri, MD, director of the Department of Prevention, Control, and Elimination of Transmissible Diseases at PAHO.
In his opening remarks, Dr. Barbosa urged the intensification of efforts with tools that are already available. These approaches include eliminating mosquito breeding sites (“80% are in or near homes”) and protecting against mosquito bites, preparing health services for early diagnosis and timely clinical management, and educating the population about dengue symptoms so they seek medical attention immediately.
Although dengue is increasing throughout Latin America and the Caribbean, the most affected countries are Brazil (83%), Paraguay (5.3%), and Argentina (3.7%), which account for 92% of the cases and 87% of the deaths, PAHO reported.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com .
The current tetravalent dengue vaccine TAK-003, from the Japanese laboratory Takeda, is not likely to control the ongoing epidemic, according to the Pan American Health Organization (PAHO). The organization emphasized the need to better understand the vaccine’s effectiveness against different serotypes and its safety under real-world clinical conditions.
The Americas are experiencing a record increase in dengue cases. Three times as many cases have been identified during 2024 (3.5 million) than were reported for the same period in 2023.
“The vaccine we have available will not curb the dengue epidemic; it should be used complementarily with other actions. The most important actions are field operations, vector control, prevention, and education,” said Daniel Salas, MD, executive manager of the PAHO Comprehensive Immunization Program, during a press conference on March 28.
“The vaccines we currently have are not the best response to reduce transmission and prevent deaths,” added Jarbas Barbosa, MD, PhD, PAHO’s director. The fatality rate remains below 0.05%, but this figure could be hard to maintain if the situation becomes more uncontrolled.
The TAK-003 regimen consists of two doses with a 3-month interval between applications, so “it is not a tool to control transmission at this moment. Studies have shown that only 8 years of [population-level] vaccination would have a significant impact on dengue transmission,” said Dr. Barbosa.
A new vaccine developed in Brazil in partnership with the company MSD, Butantan-DV, is in phase 3 trials and has the advantage of being a single-dose application, which could facilitate its use in situations with accelerated transmission. “But this vaccine will likely only be available in 2025,” said Dr. Barbosa.
PAHO officials also highlighted the need to better characterize the vaccine’s effectiveness and safety in the real world. They observed, for example, that when TAK-003 was investigated, the circulation of dengue serotype 3 was almost nonexistent, so the efficacy data against that serotype “are very limited.”
“The producer, Takeda, has very limited production capacity. Brazil is the country that uses this vaccine the most, followed by Argentina. Given that these countries have a good epidemiological surveillance system and adverse effect registration, they can conduct studies on how the vaccine performs in real life, which will greatly increase our knowledge about it. For example, we will see its effectiveness against serotype 3,” said Dr. Barbosa.
The PAHO Technical Advisory Group (TAG) on vaccine-preventable diseases recommended that any country using these vaccines have surveillance systems in place because it is important to promptly report and investigate any adverse events, said Dr. Salas. The organization also suggested that vaccination should ideally be administered in a “more controlled environment,” a phase 4 study, “to complete the safety and efficacy profile, especially in those who have not had dengue before and for dengue 3 and 4,” said Dr. Salas in response to a question from this news organization.
“People cannot expect that just because they were vaccinated, they will not get dengue. The vaccine has limited reach,” he emphasized.
Other research strategies for vector control, such as the use of the Wolbachia bacteria and mosquito sterilization, are future strategies and “not tools to control this outbreak,” noted Sylvain Aldighieri, MD, director of the Department of Prevention, Control, and Elimination of Transmissible Diseases at PAHO.
In his opening remarks, Dr. Barbosa urged the intensification of efforts with tools that are already available. These approaches include eliminating mosquito breeding sites (“80% are in or near homes”) and protecting against mosquito bites, preparing health services for early diagnosis and timely clinical management, and educating the population about dengue symptoms so they seek medical attention immediately.
Although dengue is increasing throughout Latin America and the Caribbean, the most affected countries are Brazil (83%), Paraguay (5.3%), and Argentina (3.7%), which account for 92% of the cases and 87% of the deaths, PAHO reported.
This story was translated from the Medscape Spanish edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com .
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167762</fileName> <TBEID>0C04FA9D.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FA9D</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240418T120601</QCDate> <firstPublished>20240418T145245</firstPublished> <LastPublished>20240418T145245</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240418T145244</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Matias A. Loewy</byline> <bylineText>MATÍAS A. LOEWY</bylineText> <bylineFull>MATÍAS A. LOEWY</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>The current tetravalent dengue vaccine TAK-003, from the Japanese laboratory Takeda, is not likely to control the ongoing epidemic, according to the Pan America</metaDescription> <articlePDF/> <teaserImage/> <teaser>The most important actions to take in addition to vaccination are field operations, vector control, prevention, and education.</teaser> <title>Vaccine ‘Will Not Curb’ Dengue Epidemic, Says PAHO</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>pn</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term>15</term> <term canonical="true">20</term> <term>21</term> <term>25</term> </publications> <sections> <term canonical="true">39313</term> </sections> <topics> <term>234</term> <term>311</term> <term>316</term> <term canonical="true">317</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Vaccine ‘Will Not Curb’ Dengue Epidemic, Says PAHO</title> <deck/> </itemMeta> <itemContent> <p>The current tetravalent <span class="Hyperlink"><a href="https://reference.medscape.com/drug/dengvaxia-dengue-vaccine-1000308">dengue vaccine</a></span> TAK-003, from the Japanese laboratory Takeda, is not likely to control the ongoing epidemic, according to the Pan American Health Organization (PAHO). The organization emphasized the need to better understand the vaccine’s effectiveness against different serotypes and its safety under real-world clinical conditions.</p> <p>The Americas are experiencing a record increase in dengue cases. Three times as many cases have been identified during 2024 (3.5 million) than were reported for the same period in 2023. <br/><br/>“The vaccine we have available will not curb the dengue epidemic; it should be used complementarily with other actions. The most important actions are field operations, vector control, prevention, and education,” said Daniel Salas, MD, executive manager of the PAHO Comprehensive Immunization Program, during a <span class="Hyperlink"><a href="https://www.youtube.com/watch?v=Ivlu_L1YfrQ">press conference</a></span> on March 28.<br/><br/>“The vaccines we currently have are not the best response to reduce transmission and prevent deaths,” added Jarbas Barbosa, MD, PhD, PAHO’s director. The fatality rate remains below 0.05%, but this figure could be hard to maintain if the situation becomes more uncontrolled.<br/><br/>The TAK-003 regimen consists of two doses with a 3-month interval between applications, so “it is not a tool to control transmission at this moment. Studies have shown that only 8 years of [population-level] vaccination would have a significant impact on dengue transmission,” said Dr. Barbosa.<br/><br/>A new vaccine developed in Brazil in partnership with the company MSD, Butantan-DV, is in phase 3 trials and has the advantage of being a single-dose application, which could facilitate its use in situations with accelerated transmission. “But this vaccine will likely only be available in 2025,” said Dr. Barbosa.<br/><br/>PAHO officials also highlighted the need to better characterize the vaccine’s effectiveness and safety in the real world. They observed, for example, that when TAK-003 was investigated, the circulation of dengue serotype 3 was almost nonexistent, so the efficacy data against that serotype “are very limited.”<br/><br/>“The producer, Takeda, has very limited production capacity. Brazil is the country that uses this vaccine the most, followed by Argentina. Given that these countries have a good epidemiological surveillance system and adverse effect registration, they can conduct studies on how the vaccine performs in real life, which will greatly increase our knowledge about it. For example, we will see its effectiveness against serotype 3,” said Dr. Barbosa.<br/><br/>The PAHO Technical Advisory Group (TAG) on vaccine-preventable diseases recommended that any country using these vaccines have surveillance systems in place because it is important to promptly report and investigate any adverse events, said Dr. Salas. The organization also suggested that vaccination should ideally be administered in a “more controlled environment,” a phase 4 study, “to complete the safety and efficacy profile, especially in those who have not had dengue before and for dengue 3 and 4,” said Dr. Salas in response to a question from this news organization.<br/><br/>“People cannot expect that just because they were vaccinated, they will not get dengue. The vaccine has limited reach,” he emphasized.<br/><br/>Other research strategies for vector control, such as the use of the <span class="Emphasis">Wolbachia</span> bacteria and mosquito sterilization, are future strategies and “not tools to control this outbreak,” noted Sylvain Aldighieri, MD, director of the Department of Prevention, Control, and Elimination of Transmissible Diseases at PAHO.<br/><br/>In his opening remarks, Dr. Barbosa urged the intensification of efforts with tools that are already available. These approaches include eliminating mosquito breeding sites (“80% are in or near homes”) and protecting against mosquito bites, preparing health services for early diagnosis and timely clinical management, and educating the population about dengue symptoms so they seek medical attention immediately.<br/><br/>Although dengue is increasing throughout Latin America and the Caribbean, the most affected countries are Brazil (83%), Paraguay (5.3%), and Argentina (3.7%), which account for 92% of the cases and 87% of the deaths, <span class="Hyperlink"><a href="https://www.paho.org/es/noticias/28-3-2024-ops-llama-accion-colectiva-ante-aumento-record-casos-dengue-americas">PAHO reported</a></span>.<span class="end"/></p> <p> <em> <span class="Emphasis">This story was translated from the <a href="https://espanol.medscape.com/verarticulo/5912228">Medscape Spanish edition</a> using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on </span> <span class="Hyperlink"> <a href="https://www.medscape.com/viewarticle/vaccine-will-not-curb-dengue-epidemic-says-paho-2024a1000705?src=">Medscape.com</a> </span> <span class="Emphasis">.</span> </em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
FDA Approves AI Diagnostic Tool for Early Sepsis Detection
The US Food and Drug Administration (FDA) has approved a medical device named the Sepsis ImmunoScore, which is an artificial intelligence/machine learning software, to guide rapid diagnosis and prediction of sepsis. The authorization was granted through the FDA’s De Novo pathway.
Sepsis is a complex condition, so diagnosing it early is difficult and has been a decades-long challenge for the US healthcare system.
Using both biomarkers and clinical data with the assistance of AI, the Sepsis ImmunoScore helps assess the risk for the presence of or progression to sepsis within 24 hours of patient evaluation in the emergency department or hospital. By considering 22 diverse parameters, the AI-powered tool provides a comprehensive evaluation of the patient’s biological condition, resulting in a risk score and categorization into four distinct risk levels.
It’s important to note that this system is not an alert mechanism. These risk categories are correlated with the risk for patient deterioration, including length of hospital stay, in-hospital mortality, and the need for escalated care within 24 hours (such as intensive care unit admission, mechanical ventilation, or vasopressor use). The diagnostic software is integrated directly into hospital electronic medical records.
This is the first AI diagnostic tool for sepsis to receive marketing authorization from the FDA.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a medical device named the Sepsis ImmunoScore, which is an artificial intelligence/machine learning software, to guide rapid diagnosis and prediction of sepsis. The authorization was granted through the FDA’s De Novo pathway.
Sepsis is a complex condition, so diagnosing it early is difficult and has been a decades-long challenge for the US healthcare system.
Using both biomarkers and clinical data with the assistance of AI, the Sepsis ImmunoScore helps assess the risk for the presence of or progression to sepsis within 24 hours of patient evaluation in the emergency department or hospital. By considering 22 diverse parameters, the AI-powered tool provides a comprehensive evaluation of the patient’s biological condition, resulting in a risk score and categorization into four distinct risk levels.
It’s important to note that this system is not an alert mechanism. These risk categories are correlated with the risk for patient deterioration, including length of hospital stay, in-hospital mortality, and the need for escalated care within 24 hours (such as intensive care unit admission, mechanical ventilation, or vasopressor use). The diagnostic software is integrated directly into hospital electronic medical records.
This is the first AI diagnostic tool for sepsis to receive marketing authorization from the FDA.
A version of this article appeared on Medscape.com.
The US Food and Drug Administration (FDA) has approved a medical device named the Sepsis ImmunoScore, which is an artificial intelligence/machine learning software, to guide rapid diagnosis and prediction of sepsis. The authorization was granted through the FDA’s De Novo pathway.
Sepsis is a complex condition, so diagnosing it early is difficult and has been a decades-long challenge for the US healthcare system.
Using both biomarkers and clinical data with the assistance of AI, the Sepsis ImmunoScore helps assess the risk for the presence of or progression to sepsis within 24 hours of patient evaluation in the emergency department or hospital. By considering 22 diverse parameters, the AI-powered tool provides a comprehensive evaluation of the patient’s biological condition, resulting in a risk score and categorization into four distinct risk levels.
It’s important to note that this system is not an alert mechanism. These risk categories are correlated with the risk for patient deterioration, including length of hospital stay, in-hospital mortality, and the need for escalated care within 24 hours (such as intensive care unit admission, mechanical ventilation, or vasopressor use). The diagnostic software is integrated directly into hospital electronic medical records.
This is the first AI diagnostic tool for sepsis to receive marketing authorization from the FDA.
A version of this article appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167761</fileName> <TBEID>0C04FA9C.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FA9C</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240418T115923</QCDate> <firstPublished>20240418T125618</firstPublished> <LastPublished>20240418T125618</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240418T125618</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Deepa Varma</byline> <bylineText>DEEPA VARMA</bylineText> <bylineFull>DEEPA VARMA</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>The US Food and Drug Administration (FDA) has approved a medical device named the Sepsis ImmunoScore, which is an artificial intelligence/machine learning softw</metaDescription> <articlePDF/> <teaserImage/> <teaser>Using both biomarkers and clinical data with the assistance of AI, the Sepsis ImmunoScore helps assess the risk for the presence of or progression to sepsis within 24 hours.</teaser> <title>FDA Approves AI Diagnostic Tool for Early Sepsis Detection</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>mdemed</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> <journalTitle/> <journalFullTitle/> <copyrightStatement/> </publicationData> </publications_g> <publications> <term>15</term> <term>20</term> <term canonical="true">21</term> <term>58877</term> </publications> <sections> <term>27979</term> <term canonical="true">39313</term> </sections> <topics> <term canonical="true">234</term> <term>319</term> <term>315</term> <term>288</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>FDA Approves AI Diagnostic Tool for Early Sepsis Detection</title> <deck/> </itemMeta> <itemContent> <p>The US Food and Drug Administration (FDA) has approved a medical device named the <span class="Hyperlink">Sepsis</span> ImmunoScore, which is an artificial intelligence/machine learning software, to guide rapid diagnosis and prediction of sepsis. The authorization was granted through the FDA’s <span class="Hyperlink"><a href="https://www.fda.gov/medical-devices/premarket-submissions-selecting-and-preparing-correct-submission/de-novo-classification-request">De Novo pathway</a></span>.</p> <p>Sepsis is a complex condition, so diagnosing it early is difficult and has been a decades-long challenge for the US healthcare system.<br/><br/>Using both biomarkers and clinical data with the assistance of AI, the Sepsis ImmunoScore helps assess the risk for the presence of or progression to sepsis within 24 hours of patient evaluation in the emergency department or hospital. By considering 22 diverse parameters, the AI-powered tool provides a comprehensive evaluation of the patient’s biological condition, resulting in a risk score and categorization into four distinct risk levels.<br/><br/>It’s important to note that this system is not an alert mechanism. These risk categories are correlated with the risk for patient deterioration, including length of hospital stay, in-hospital mortality, and the need for escalated care within 24 hours (such as intensive care unit admission, <span class="Hyperlink"><a href="https://emedicine.medscape.com/article/304068-overview">mechanical ventilation</a></span>, or vasopressor use). The diagnostic software is integrated directly into hospital electronic medical records.<br/><br/>This is the first AI diagnostic tool for sepsis to receive marketing authorization from the FDA.<span class="end"/></p> <p> <em>A version of this article appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/fda-approves-ai-diagnostic-tool-early-sepsis-detection-2024a100074d?src=">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
Diabetic Foot Ulcers: Life-Threatening Issue in Need of Help
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”
The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.
This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.
This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.
Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown to help heal wounds and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.
Worldwide, about 18.6 million people have a DFU each year, including 1.6 million in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and DFUs are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.
While the statistics paint a grim picture, progress is being made on several fronts:
- US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.
- New treatments are under study.
- A multidisciplinary team approach is known to improve outcomes.
Anatomy of a DFU
When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”
A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.
About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the American Limb Preservation Society, which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.
FDA Guidance on Drug Development for DFIs
In October, the FDA issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the guidance, which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.
According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”
The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct costs of care for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.
Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”
Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.
Treatments: Current, Under Study
Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.
More options are needed, Dr. Armstrong said.
Among the many approaches under study:
- DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.
- After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (P = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (P = .03).
- An closed more DFUs than standard care after 12 weeks — 70% vs 34% (P = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).
- A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (P = .021, unadjusted).
- Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.
The Power of a Team
Multidisciplinary approaches to treatment are effective in reducing amputation, with one review of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”
Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.
Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service launched in 2012 and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.
“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”
“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”
While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”
The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “all feet on deck” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.
Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “Knock your socks off” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.
Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).
A version of this article first appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167748</fileName> <TBEID>0C04FA51.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FA51</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240417T213506</QCDate> <firstPublished>20240418T112848</firstPublished> <LastPublished>20240418T112848</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240418T112848</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>KATHLEEN DOHENY</byline> <bylineText>KATHLEEN DOHENY</bylineText> <bylineFull>KATHLEEN DOHENY</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better t</metaDescription> <articlePDF/> <teaserImage/> <teaser>The 5-year mortality rate for diabetic foot ulcers is 30%, but it climbs to 70% after amputation. </teaser> <title>Diabetic Foot Ulcers: Life-Threatening Issue in Need of Help</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>endo</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>skin</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>mdsurg</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> <journalTitle/> <journalFullTitle/> <copyrightStatement>2018 Frontline Medical Communications Inc.,</copyrightStatement> </publicationData> </publications_g> <publications> <term>34</term> <term>13</term> <term>15</term> <term>21</term> <term canonical="true">52226</term> </publications> <sections> <term>27980</term> <term canonical="true">39313</term> </sections> <topics> <term canonical="true">205</term> <term>39212</term> <term>234</term> <term>212</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Diabetic Foot Ulcers: Life-Threatening Issue in Need of Help</title> <deck/> </itemMeta> <itemContent> <p>The photo of the patient’s foot, sent from his campsite, included a cheeky note: “I remember you telling me that getting in trouble doing something was better than getting in trouble doing nothing. This lets me get out there and know that I have feedback.”</p> <p>The “this” was the patient’s “foot selfie,” an approach that allows patients at a risk for diabetic foot ulcers (DFUs) to snap a picture and send it to their healthcare providers for evaluation.<br/><br/>This particular patient had an extensive history of previous wounds. Some had essentially kept him house-bound in the past, as he was afraid to get another one.<br/><br/>This time, however, he got an all-clear to keep on camping, “and we scheduled him in on the following Tuesday [for follow-up],” said the camper’s physician David G. Armstrong, DPM, MD, PhD, professor of surgery and neurological surgery, USC Keck School of Medicine, Los Angeles.<br/><br/>Dr. Armstrong is one of the researchers evaluating the concept of foot selfies. It’s a welcome advance, he and others said, and has been shown <a href="https://journals.sagepub.com/doi/full/10.1177/19322968211053348">to help heal wounds</a> and reverse pre-ulcer lesions. Research on foot selfies continues, but much more is needed to solve the issue of DFUs, diabetic foot infections (DFIs), and the high rates of reinfection, experts know.<br/><br/>Worldwide, about 18.6 million people have a DFU each year, including <a href="https://jamanetwork.com/journals/jama/article-abstract/2806655">1.6 million</a> in the United States. About 50%-60% of ulcers become infected, with 20% of moderate to severe infections requiring amputation of the limb. The 5-year mortality rate for DFUs is 30%, but it climbs to 70% after amputation. While about 40% of ulcers heal within 12 weeks, 42% recur at the 1-year mark, setting up a vicious and costly cycle. Healthcare costs for patients with diabetes and <a href="https://bmchealthservres.biomedcentral.com/articles/10.1186/s12913-024-10873-9">DFUs</a> are five times as high as costs for patients with diabetes but no DFUs. The per capita cost to treat a DFU in America is $17,500.<br/><br/>While the statistics paint a grim picture, progress is being made on several fronts:</p> <ul class="body"> <li>US Food and Drug Administration (FDA) guidance on the development of drugs for DFUs, under evaluation, is forthcoming.</li> <li>New treatments are under study.</li> <li>A multidisciplinary team approach is known to improve outcomes.</li> </ul> <h2>Anatomy of a DFU</h2> <p>When neuropathy develops in those with diabetes, they no longer have what Dr. Armstrong calls the “gift” of pain perception. “They can wear a hole in their foot like you and I wear a hole in our sock or shoe,” he said. “That hole is called a diabetic foot ulcer.”</p> <p>A DFU is an open wound on the foot, often occurring when bleeding develops beneath a callus and then the callus wears away. Deeper tissues of the foot are then exposed.<br/><br/>About half of the DFUs get infected, hence the FDA guidance, said Dr. Armstrong, who is also founding president of the <a href="https://limbpreservationsociety.org/">American Limb Preservation Society,</a> which aims to eliminate preventable amputations within the next generation. Every 20 seconds, Dr. Armstrong said, someone in the world loses a leg due to diabetes.<br/><br/></p> <h2>FDA Guidance on Drug Development for DFIs</h2> <p>In October, the <a href="https://www.fda.gov/regulatory-information/search-fda-guidance-documents/diabetic-foot-infections-developing-drugs-treatment">FDA</a> issued draft guidance for industry to articulate the design of clinical trials for developing antibacterial drugs to treat DFIs without concomitant bone and joint involvement. Comments closed on December 18. Among the points in the <a href="https://www.fda.gov/media/173006/download">guidance,</a> which is nonbinding, are to include DFIs of varying depths and extent in phase 3 trials and ideally to include only those patients who have not had prior antibacterial treatment for the current DFI.</p> <p>According to an FDA spokesperson, “The agency is working to finalize the guidance. However, a timeline for its release has not yet been established.”<br/><br/>The good news about the upcoming FDA guidance, Dr. Armstrong said, is that the agency has realized the importance of treating the infections. Fully one third of direct <a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7092527/">costs of care</a> for diabetes are spent on the lower extremities, he said. Keeping patients out of the hospital, uninfected, and “keeping legs on bodies” are all important goals, he said.<br/><br/>Pharmaceutical firms need to understand that “you aren’t dealing with a normal ulcer,” said Andrew J.M. Boulton, MD, professor of medicine at the University of Manchester and physician consultant at the Manchester Royal Infirmary, Manchester, England, and a visiting professor at the University of Miami. For research, “the most important thing is to take account of off-loading the ulcers,” he said. “Most ulcers will heal if put in a boot.”<br/><br/>Dr. Boulton, like Dr. Armstrong, a long-time expert in the field, contended that pharma has not understood this concept and has wasted millions over the last three decades doing studies that were poorly designed and controlled.<br/><br/></p> <h2>Treatments: Current, Under Study</h2> <p>Currently, DFIs are treated with antimicrobial therapy, without or without debridement, along with a clinical assessment for ischemia. If ischemia is found, care progresses to wound care and off-loading devices, such as healing sandals. Clinicians then assess the likelihood of improved outcomes with revascularization based on operative risks and distribution of lower extremity artery disease and proceed depending on the likelihood. If osteomyelitis testing shows it is present, providers proceed to wound debridement, limb-sparing amputation, and prolonged antimicrobials, as needed.</p> <p>More options are needed, Dr. Armstrong said.<br/><br/>Among the many approaches under study:</p> <ul class="body"> <li>DFUs can be accurately detected by applying artificial intelligence to the “foot selfie” images taken by patients on smartphones, research by Dr. and has found.</li> <li>After a phase 3 study of for DFUs originally intending to enroll 300 subjects was discontinued because of slow patient recruitment, an interim analysis was conducted on 44 participants. It showed a positive trend toward wound closure in the group receiving the injected gene therapy, VM202 (ENGENSIS), in their calf muscles. VM202 is a plasmid DNA-encoding human hepatocyte growth factor. While those in both the intervention and placebo groups showed wound-closing effects at month 6, in 23 patients with neuro-ischemic ulcers, the percentage of those reaching complete closure of the DFU was significantly higher in the treated group at months 3, 4, and 5 (<em>P</em> = .0391, .0391, and .0361, respectively). After excluding two outliers, the difference in months 3-6 became more significant (<em>P</em> = .03).</li> <li>An closed more DFUs than standard care after 12 weeks — 70% vs 34% (<em>P</em> = .00032). Of the 100 participants randomized, 50 per group, 42% of the treatment group and 56% of the control group experienced adverse events, with eight withdrawn due to serious adverse events (such as osteomyelitis).</li> <li>A closed more refractory DFUs over a 16-week study than standard sharp debridement, with 65% of water-treated ulcers healed but just 42% of the standard care group (<em>P</em> = .021, unadjusted).</li> <li>Researchers from UC Davis and VA Northern California Healthcare are evaluating timolol, a beta adrenergic receptor blocker already approved for topical administration for glaucoma, as a way to heal chronic DFUs faster. After demonstrating that the medication worked in animal models, researchers then launched a study to use it off-label for DFUs. While data are still being analyzed, researcher Roslyn (Rivkah) Isseroff, MD, of UC Davis and VA, said that data so far demonstrate that the timolol reduced transepidermal water loss in the healed wounds, and that is linked with a decrease in re-ulceration.</li> </ul> <h2>The Power of a Team</h2> <p>Multidisciplinary approaches to treatment are effective in reducing amputation, with one <a href="https://www.jvascsurg.org/article/S0741-5214(19)32229-3/fulltext">review</a> of 33 studies finding the approach worked to decrease amputation in 94% of them. “The American Limb Preservation Society (ALPS) lists 30 programs,” said Dr. Armstrong, the founding president of the organization. “There may be as many as 100.”</p> <p>Team compositions vary but usually include at least one medical specialty clinician, such as infectious disease, primary care, or endocrinology, and two or more specialty clinicians, such as vascular, podiatric, orthopedic, or plastic surgery. A shoe specialist is needed to prescribe and manage footwear. Other important team members include nutrition experts and behavioral health professionals to deal with associated depression.<br/><br/>Johns Hopkins’ Multidisciplinary Diabetic Foot and Wound Service <a href="https://www.hopkinsmedicine.org/heart-vascular-institute/vascular-surgery/diabetic-wound-clinic">launched in 2012</a> and includes vascular surgeons, surgical podiatrists, endocrinologists, wound care nurses, advanced practice staff, board-certified wound care specialists, orthopedic surgeons, infection disease experts, physical therapists, and certified orthotists.<br/><br/>“This interdisciplinary care model has been repeatedly validated by research as superior for limb salvage and wound healing,” said Nestoras Mathioudakis, MD, codirector of the service. “For instance, endocrinologists and diabetes educators are crucial for managing uncontrolled diabetes — a key factor in infection and delayed wound healing. Similarly, vascular surgeons play a vital role in addressing peripheral arterial disease to improve blood flow to the affected area.”<br/><br/>“Diabetic foot ulcers might require prolonged periods of specialized care, including meticulous wound management and off-loading, overseen by surgical podiatrists and wound care experts,” he said. “In cases where infection is present, particularly with multidrug resistant organisms or when standard antibiotics are contraindicated, the insight of an infectious disease specialist is invaluable.”<br/><br/>While the makeup of teams varies from location to location, he said “the hallmark of effective teams is their ability to comprehensively manage glycemic control, foot wounds, vascular disease, and infections.”<br/><br/>The power of teams, Dr. Armstrong said, is very much evident after his weekly “foot selfie rounds” conducted Mondays at 7 AM, with an “<a href="https://diabeticfootonline.com/2020/08/09/a-foot-selfie-using-mobile-phones-for-diabetic-foot-surveillance/">all feet on deck</a>” approach. “Not a week goes by when we don’t stop a hospitalization,” he said of the team evaluating the photos, due to detecting issues early, while still in the manageable state.<br/><br/>Teams can trump technology, Dr. Armstrong said. A team of just a primary care doctor and a podiatrist can make a significant reduction in amputations, he said, just by a “<a href="https://diabeticfootonline.com/2017/11/08/knock-your-socks-off-and-prevent-diabetes-related-amputations-heres-how/">Knock your socks off</a>” approach. He reminds primary care doctors that observing the feet of their patients with diabetes can go a long way to reducing DFUs and the hospitalizations and amputations that can result.<br/><br/>Dr. Mathioudakis and Dr. Isseroff reported no disclosures. Dr. Boulton consults for Urgo Medical, Nevro Corporation, and AOT, Inc. Dr. Armstrong reported receiving consulting fees from Podimetrics; Molnlycke; Cardiovascular Systems, Inc.; Endo Pharmaceuticals; and Averitas Pharma (GRT US).<span class="end"/></p> <p> <em>A version of this article first appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/diabetic-foot-ulcers-life-threatening-issue-need-help-2024a100078r">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
4 Years In, a Sobering Look at Long COVID Progress
Four years ago in the spring of 2020, physicians and patients coined the term “long COVID” to describe a form of the viral infection from which recovery seemed impossible. (And the old nickname “long-haulers” seems so quaint now.)
What started as a pandemic that killed nearly 3 million people globally in 2020 alone would turn into a chronic disease causing a long list of symptoms — from extreme fatigue, to brain fog, tremors, nausea, headaches, rapid heartbeat, and more.
Today, 6.4% of Americans report symptoms of long COVID, and many have never recovered.
Still, we’ve come a long way, although there’s much we don’t understand about the condition. At the very least, physicians have a greater understanding that long COVID exists and can cause serious long-term symptoms.
While physicians may not have a blanket diagnostic tool that works for all patients with long COVID, they have refined existing tests for more accurate results, said Nisha Viswanathan, MD, director of the University of California Los Angeles Long COVID Program at UCLA Health.
Also, a range of new treatments, now undergoing clinical trials, have emerged that have proved effective in managing long COVID symptoms.
Catecholamine testing, for example, is now commonly used to diagnose long COVID, particularly in those who have dysautonomia, a condition caused by dysfunction of the autonomic nervous system and marked by dizziness, low blood pressure, nausea, and brain fog.
Very high levels of the neurotransmitter, for example, were shown to indicate long COVID in a January 2021 study published in the journal Clinical Medicine.
Certain biomarkers have also been shown indicative of the condition, including low serotonin levels. A study published this year in Cell found lower serotonin levels in patients with long COVID driven by low levels of circulating SARS-CoV-2, the virus that causes the condition.
Still, said Dr. Viswanathan, long COVID is a disease diagnosed by figuring out what a patient does not have — by ruling out other causes — rather than what they do. “It’s still a moving target,” she said, meaning that the disease is always changing based on the variant of acute COVID.
Promising Treatments Have Emerged
Dysautonomia, and especially the associated brain fog, fatigue, and dizziness, are now common conditions. As a result, physicians have gotten better at treating them. The vagus nerve is the main nerve of the parasympathetic nervous system that controls everything from digestion to mental health. A February 2022 pilot study suggested a link between vagus nerve dysfunction and some long COVID symptoms.
Vagus nerve stimulation is one form of treatment which involves using a device to stimulate the vagus nerve with electrical impulses. Dr. Viswanathan has been using the treatment in patients with fatigue, brain fog, anxiety, and depression — results, she contends, have been positive.
“This is something tangible that we can offer to patients,” she said.
Curative treatments for long COVID remain elusive, but doctors have many more tools for symptom management than before, said Ziyad Al-Aly, MD, a global expert on long COVID and chief of research and development at the Veterans Affairs St. Louis Health Care System.
For example, physicians are using beta-blockers to treat postural tachycardia syndrome (POTS), a symptom of long COVID that happens when the heart rate increases rapidly after someone stands up or lies down. Beta-blockers, such as the off-label medication ivabradine, have been used clinically to control heart rate, according to a March 2022 study published in the journal HeartRhythm Case Reports.
“It’s not a cure, but beta-blockers can help patients manage their symptoms,” said Dr. Al-Aly.
Additionally, some patients respond well to low-dose naltrexone for the treatment of extreme fatigue associated with long COVID. A January 2024 article in the journal Clinical Therapeutics found that fatigue symptoms improved in patients taking the medication.
Dr. Al-Aly said doctors treating patients with long COVID are getting better at pinpointing the phenotype or manifestation of the condition and diagnosing a treatment accordingly. Treating long COVID fatigue is not the same as treating POTS or symptoms of headache and joint pain.
It’s still all about the management of symptoms and doctors lack any US Food and Drug Administration–approved medications specifically for the condition.
Clinical Trials Exploring New Therapies
Still, a number of large clinical trials currently underway may change that, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
Two clinical trials headed by Dr. Putrino’s lab are looking into repurposing two HIV antivirals to see whether they affect the levels of circulating SARS-CoV-2 virus in the body that may cause long COVID. The hope is that the antivirals Truvada and maraviroc can reduce the «reactivation of latent virus» that, said Dr. Putrino, causes lingering long COVID symptoms.
Ongoing trials are looking into the promise of SARS-CoV-2 monoclonal antibodies, produced from cells made by cloning a unique white blood cell, as a treatment option. The trials are investigating whether these antibodies may similarly target viral reservoirs that are causing persistence of symptoms in some patients.
Other trials are underway through the National Institutes of Health (NIH) RECOVER initiative in which more than 17,000 patients are enrolled, the largest study of its kind, said Grace McComsey, MD.
Dr. McComsey, who leads the study at University Hospitals Health System in Cleveland, said that after following patients for up to 4 years researchers have gathered “a massive repository of information” they hope will help scientists crack the code of this very complex disease.
She and other RECOVER researchers have recently published studies on a variety of findings, reporting in February, for example, that COVID infections may trigger other autoimmune diseases such as rheumatoid arthritis and type 2 diabetes. Another recent finding showed that people with HIV are at a higher risk for complications due to acute COVID-19.
Lack of Urgency Holds Back Progress
Still, others like Dr. Al-Aly and Dr. Putrino felt that the initiative isn’t moving fast enough. Dr. Al-Aly said that the NIH needs to “get its act together” and do more for long COVID. In the future, he said that we need to double down on our efforts to expand funding and increase urgency to better understand the mechanism of disease, risk factors, and treatments, as well as societal and economic implications.
“We did trials for COVID-19 vaccines at warp speed, but we’re doing trials for long COVID at a snail’s pace,” he said.
Dr. Al-Aly is concerned about the chronic nature of the disease and how it affects patients down the line. His large-scale study published last month in the journal Science looked specifically at chronic fatigue syndrome triggered by the infection and its long-term impact on patients.
He’s concerned about the practical implications for people who are weighted down with symptoms for multiple years.
“Being fatigued and ill for a few months is one thing, but being at home for 5 years is a totally different ballgame.”
A version of this article first appeared on Medscape.com.
Four years ago in the spring of 2020, physicians and patients coined the term “long COVID” to describe a form of the viral infection from which recovery seemed impossible. (And the old nickname “long-haulers” seems so quaint now.)
What started as a pandemic that killed nearly 3 million people globally in 2020 alone would turn into a chronic disease causing a long list of symptoms — from extreme fatigue, to brain fog, tremors, nausea, headaches, rapid heartbeat, and more.
Today, 6.4% of Americans report symptoms of long COVID, and many have never recovered.
Still, we’ve come a long way, although there’s much we don’t understand about the condition. At the very least, physicians have a greater understanding that long COVID exists and can cause serious long-term symptoms.
While physicians may not have a blanket diagnostic tool that works for all patients with long COVID, they have refined existing tests for more accurate results, said Nisha Viswanathan, MD, director of the University of California Los Angeles Long COVID Program at UCLA Health.
Also, a range of new treatments, now undergoing clinical trials, have emerged that have proved effective in managing long COVID symptoms.
Catecholamine testing, for example, is now commonly used to diagnose long COVID, particularly in those who have dysautonomia, a condition caused by dysfunction of the autonomic nervous system and marked by dizziness, low blood pressure, nausea, and brain fog.
Very high levels of the neurotransmitter, for example, were shown to indicate long COVID in a January 2021 study published in the journal Clinical Medicine.
Certain biomarkers have also been shown indicative of the condition, including low serotonin levels. A study published this year in Cell found lower serotonin levels in patients with long COVID driven by low levels of circulating SARS-CoV-2, the virus that causes the condition.
Still, said Dr. Viswanathan, long COVID is a disease diagnosed by figuring out what a patient does not have — by ruling out other causes — rather than what they do. “It’s still a moving target,” she said, meaning that the disease is always changing based on the variant of acute COVID.
Promising Treatments Have Emerged
Dysautonomia, and especially the associated brain fog, fatigue, and dizziness, are now common conditions. As a result, physicians have gotten better at treating them. The vagus nerve is the main nerve of the parasympathetic nervous system that controls everything from digestion to mental health. A February 2022 pilot study suggested a link between vagus nerve dysfunction and some long COVID symptoms.
Vagus nerve stimulation is one form of treatment which involves using a device to stimulate the vagus nerve with electrical impulses. Dr. Viswanathan has been using the treatment in patients with fatigue, brain fog, anxiety, and depression — results, she contends, have been positive.
“This is something tangible that we can offer to patients,” she said.
Curative treatments for long COVID remain elusive, but doctors have many more tools for symptom management than before, said Ziyad Al-Aly, MD, a global expert on long COVID and chief of research and development at the Veterans Affairs St. Louis Health Care System.
For example, physicians are using beta-blockers to treat postural tachycardia syndrome (POTS), a symptom of long COVID that happens when the heart rate increases rapidly after someone stands up or lies down. Beta-blockers, such as the off-label medication ivabradine, have been used clinically to control heart rate, according to a March 2022 study published in the journal HeartRhythm Case Reports.
“It’s not a cure, but beta-blockers can help patients manage their symptoms,” said Dr. Al-Aly.
Additionally, some patients respond well to low-dose naltrexone for the treatment of extreme fatigue associated with long COVID. A January 2024 article in the journal Clinical Therapeutics found that fatigue symptoms improved in patients taking the medication.
Dr. Al-Aly said doctors treating patients with long COVID are getting better at pinpointing the phenotype or manifestation of the condition and diagnosing a treatment accordingly. Treating long COVID fatigue is not the same as treating POTS or symptoms of headache and joint pain.
It’s still all about the management of symptoms and doctors lack any US Food and Drug Administration–approved medications specifically for the condition.
Clinical Trials Exploring New Therapies
Still, a number of large clinical trials currently underway may change that, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
Two clinical trials headed by Dr. Putrino’s lab are looking into repurposing two HIV antivirals to see whether they affect the levels of circulating SARS-CoV-2 virus in the body that may cause long COVID. The hope is that the antivirals Truvada and maraviroc can reduce the «reactivation of latent virus» that, said Dr. Putrino, causes lingering long COVID symptoms.
Ongoing trials are looking into the promise of SARS-CoV-2 monoclonal antibodies, produced from cells made by cloning a unique white blood cell, as a treatment option. The trials are investigating whether these antibodies may similarly target viral reservoirs that are causing persistence of symptoms in some patients.
Other trials are underway through the National Institutes of Health (NIH) RECOVER initiative in which more than 17,000 patients are enrolled, the largest study of its kind, said Grace McComsey, MD.
Dr. McComsey, who leads the study at University Hospitals Health System in Cleveland, said that after following patients for up to 4 years researchers have gathered “a massive repository of information” they hope will help scientists crack the code of this very complex disease.
She and other RECOVER researchers have recently published studies on a variety of findings, reporting in February, for example, that COVID infections may trigger other autoimmune diseases such as rheumatoid arthritis and type 2 diabetes. Another recent finding showed that people with HIV are at a higher risk for complications due to acute COVID-19.
Lack of Urgency Holds Back Progress
Still, others like Dr. Al-Aly and Dr. Putrino felt that the initiative isn’t moving fast enough. Dr. Al-Aly said that the NIH needs to “get its act together” and do more for long COVID. In the future, he said that we need to double down on our efforts to expand funding and increase urgency to better understand the mechanism of disease, risk factors, and treatments, as well as societal and economic implications.
“We did trials for COVID-19 vaccines at warp speed, but we’re doing trials for long COVID at a snail’s pace,” he said.
Dr. Al-Aly is concerned about the chronic nature of the disease and how it affects patients down the line. His large-scale study published last month in the journal Science looked specifically at chronic fatigue syndrome triggered by the infection and its long-term impact on patients.
He’s concerned about the practical implications for people who are weighted down with symptoms for multiple years.
“Being fatigued and ill for a few months is one thing, but being at home for 5 years is a totally different ballgame.”
A version of this article first appeared on Medscape.com.
Four years ago in the spring of 2020, physicians and patients coined the term “long COVID” to describe a form of the viral infection from which recovery seemed impossible. (And the old nickname “long-haulers” seems so quaint now.)
What started as a pandemic that killed nearly 3 million people globally in 2020 alone would turn into a chronic disease causing a long list of symptoms — from extreme fatigue, to brain fog, tremors, nausea, headaches, rapid heartbeat, and more.
Today, 6.4% of Americans report symptoms of long COVID, and many have never recovered.
Still, we’ve come a long way, although there’s much we don’t understand about the condition. At the very least, physicians have a greater understanding that long COVID exists and can cause serious long-term symptoms.
While physicians may not have a blanket diagnostic tool that works for all patients with long COVID, they have refined existing tests for more accurate results, said Nisha Viswanathan, MD, director of the University of California Los Angeles Long COVID Program at UCLA Health.
Also, a range of new treatments, now undergoing clinical trials, have emerged that have proved effective in managing long COVID symptoms.
Catecholamine testing, for example, is now commonly used to diagnose long COVID, particularly in those who have dysautonomia, a condition caused by dysfunction of the autonomic nervous system and marked by dizziness, low blood pressure, nausea, and brain fog.
Very high levels of the neurotransmitter, for example, were shown to indicate long COVID in a January 2021 study published in the journal Clinical Medicine.
Certain biomarkers have also been shown indicative of the condition, including low serotonin levels. A study published this year in Cell found lower serotonin levels in patients with long COVID driven by low levels of circulating SARS-CoV-2, the virus that causes the condition.
Still, said Dr. Viswanathan, long COVID is a disease diagnosed by figuring out what a patient does not have — by ruling out other causes — rather than what they do. “It’s still a moving target,” she said, meaning that the disease is always changing based on the variant of acute COVID.
Promising Treatments Have Emerged
Dysautonomia, and especially the associated brain fog, fatigue, and dizziness, are now common conditions. As a result, physicians have gotten better at treating them. The vagus nerve is the main nerve of the parasympathetic nervous system that controls everything from digestion to mental health. A February 2022 pilot study suggested a link between vagus nerve dysfunction and some long COVID symptoms.
Vagus nerve stimulation is one form of treatment which involves using a device to stimulate the vagus nerve with electrical impulses. Dr. Viswanathan has been using the treatment in patients with fatigue, brain fog, anxiety, and depression — results, she contends, have been positive.
“This is something tangible that we can offer to patients,” she said.
Curative treatments for long COVID remain elusive, but doctors have many more tools for symptom management than before, said Ziyad Al-Aly, MD, a global expert on long COVID and chief of research and development at the Veterans Affairs St. Louis Health Care System.
For example, physicians are using beta-blockers to treat postural tachycardia syndrome (POTS), a symptom of long COVID that happens when the heart rate increases rapidly after someone stands up or lies down. Beta-blockers, such as the off-label medication ivabradine, have been used clinically to control heart rate, according to a March 2022 study published in the journal HeartRhythm Case Reports.
“It’s not a cure, but beta-blockers can help patients manage their symptoms,” said Dr. Al-Aly.
Additionally, some patients respond well to low-dose naltrexone for the treatment of extreme fatigue associated with long COVID. A January 2024 article in the journal Clinical Therapeutics found that fatigue symptoms improved in patients taking the medication.
Dr. Al-Aly said doctors treating patients with long COVID are getting better at pinpointing the phenotype or manifestation of the condition and diagnosing a treatment accordingly. Treating long COVID fatigue is not the same as treating POTS or symptoms of headache and joint pain.
It’s still all about the management of symptoms and doctors lack any US Food and Drug Administration–approved medications specifically for the condition.
Clinical Trials Exploring New Therapies
Still, a number of large clinical trials currently underway may change that, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.
Two clinical trials headed by Dr. Putrino’s lab are looking into repurposing two HIV antivirals to see whether they affect the levels of circulating SARS-CoV-2 virus in the body that may cause long COVID. The hope is that the antivirals Truvada and maraviroc can reduce the «reactivation of latent virus» that, said Dr. Putrino, causes lingering long COVID symptoms.
Ongoing trials are looking into the promise of SARS-CoV-2 monoclonal antibodies, produced from cells made by cloning a unique white blood cell, as a treatment option. The trials are investigating whether these antibodies may similarly target viral reservoirs that are causing persistence of symptoms in some patients.
Other trials are underway through the National Institutes of Health (NIH) RECOVER initiative in which more than 17,000 patients are enrolled, the largest study of its kind, said Grace McComsey, MD.
Dr. McComsey, who leads the study at University Hospitals Health System in Cleveland, said that after following patients for up to 4 years researchers have gathered “a massive repository of information” they hope will help scientists crack the code of this very complex disease.
She and other RECOVER researchers have recently published studies on a variety of findings, reporting in February, for example, that COVID infections may trigger other autoimmune diseases such as rheumatoid arthritis and type 2 diabetes. Another recent finding showed that people with HIV are at a higher risk for complications due to acute COVID-19.
Lack of Urgency Holds Back Progress
Still, others like Dr. Al-Aly and Dr. Putrino felt that the initiative isn’t moving fast enough. Dr. Al-Aly said that the NIH needs to “get its act together” and do more for long COVID. In the future, he said that we need to double down on our efforts to expand funding and increase urgency to better understand the mechanism of disease, risk factors, and treatments, as well as societal and economic implications.
“We did trials for COVID-19 vaccines at warp speed, but we’re doing trials for long COVID at a snail’s pace,” he said.
Dr. Al-Aly is concerned about the chronic nature of the disease and how it affects patients down the line. His large-scale study published last month in the journal Science looked specifically at chronic fatigue syndrome triggered by the infection and its long-term impact on patients.
He’s concerned about the practical implications for people who are weighted down with symptoms for multiple years.
“Being fatigued and ill for a few months is one thing, but being at home for 5 years is a totally different ballgame.”
A version of this article first appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167747</fileName> <TBEID>0C04FA4F.SIG</TBEID> <TBUniqueIdentifier>MD_0C04FA4F</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname/> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240417T212940</QCDate> <firstPublished>20240418T103604</firstPublished> <LastPublished>20240418T103604</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240418T103604</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Sara Novak</byline> <bylineText>SARA NOVAK</bylineText> <bylineFull>SARA NOVAK</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType/> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>Four years ago in the spring of 2020, physicians and patients coined the term “long COVID” to describe a form of the viral infection from which recovery seemed </metaDescription> <articlePDF/> <teaserImage/> <teaser>Long COVID is still a disease diagnosed by figuring out what a patient does not have. Symptom management is the only treatment now.</teaser> <title>4 Years In, a Sobering Look at Long COVID Progress</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear/> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>fp</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>idprac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>im</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>icymicov</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> <publicationData> <publicationCode>chph</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> </publicationData> </publications_g> <publications> <term>15</term> <term>20</term> <term canonical="true">21</term> <term>69586</term> <term>6</term> </publications> <sections> <term>26933</term> <term>27980</term> <term canonical="true">39313</term> </sections> <topics> <term canonical="true">72046</term> <term>63993</term> <term>234</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>4 Years In, a Sobering Look at Long COVID Progress</title> <deck/> </itemMeta> <itemContent> <p>Four years ago in the <a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7992371/%2523:~:text=%2525E2%252580%25259CLong%252520COVID%2525E2%252580%25259D%252520is%252520the%252520condition,19,%252520whether%252520tested%252520or%252520not.&text=The%252520name%252520%2525E2%252580%25259Clong%252520COVID%2525E2%252580%25259D%252520was,their%252520journeys%252520of%252520not%252520recovering.">spring of 2020</a>, physicians and patients coined the term “long COVID” to describe a form of the viral infection from which recovery seemed impossible. (And the old nickname “long-haulers” seems so quaint now.)</p> <p>What started as a pandemic that killed nearly <a href="https://www.who.int/data/stories/the-true-death-toll-of-covid-19-estimating-global-excess-mortality">3 million people</a> globally in 2020 alone would turn into a chronic disease causing a long list of symptoms — from extreme fatigue, to brain fog, tremors, nausea, headaches, rapid heartbeat, and more.<br/><br/>Today, <a href="https://www.cdc.gov/mmwr/volumes/73/wr/mm7306a4.htm">6.4%</a> of Americans report symptoms of long COVID, and many have never recovered.<br/><br/>Still, we’ve come a long way, although there’s much we don’t understand about the condition. At the very least, physicians have a greater understanding that long COVID exists and can cause serious long-term symptoms.<br/><br/>While physicians may not have a blanket diagnostic tool that works for all patients with long COVID, they have refined existing tests for more accurate results, said Nisha Viswanathan, MD, director of the University of California Los Angeles Long COVID Program at UCLA Health.<br/><br/>Also, a range of new treatments, now undergoing clinical trials, have emerged that have proved effective in managing long COVID symptoms.<br/><br/>Catecholamine testing, for example, is now commonly used to diagnose long COVID, particularly in those who have dysautonomia, a condition caused by dysfunction of the autonomic nervous system and marked by dizziness, low blood pressure, nausea, and brain fog.<br/><br/>Very high levels of the neurotransmitter, for example, were shown to indicate long COVID in a January 2021 study published in the journal <em><a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7850225/">Clinical Medicine</a></em>.<br/><br/>Certain biomarkers have also been shown indicative of the condition, including low serotonin levels. A study published this year in <em><a href="https://www.cell.com/cell/fulltext/S0092-8674(23)01034-6?_returnURL=https://linkinghub.elsevier.com/retrieve/pii/S0092867423010346?showall=true">Cell</a></em> found lower serotonin levels in patients with long COVID driven by low levels of circulating SARS-CoV-2, the virus that causes the condition.<br/><br/>Still, said Dr. Viswanathan, long COVID is a disease diagnosed by figuring out what a patient does not have — by ruling out other causes — rather than what they do. “It’s still a moving target,” she said, meaning that the disease is always changing based on the variant of acute COVID.<br/><br/></p> <h2>Promising Treatments Have Emerged</h2> <p>Dysautonomia, and especially the associated brain fog, fatigue, and dizziness, are now common conditions. As a result, physicians have gotten better at treating them. The vagus nerve is the main nerve of the parasympathetic nervous system that controls everything from digestion to mental health. A February 2022 <a href="https://www.eurekalert.org/news-releases/943102">pilot</a> study suggested a link between vagus nerve dysfunction and some long COVID symptoms.</p> <p>Vagus nerve stimulation is one form of treatment which involves using a device to stimulate the vagus nerve with electrical impulses. Dr. Viswanathan has been using the treatment in patients with fatigue, brain fog, anxiety, and <a href="https://emedicine.medscape.com/article/286759-overview">depression</a> — results, she contends, have been positive.<br/><br/>“This is something tangible that we can offer to patients,” she said.<br/><br/>Curative treatments for long COVID remain elusive, but doctors have many more tools for symptom management than before, said Ziyad Al-Aly, MD, a global expert on long COVID and chief of research and development at the Veterans Affairs St. Louis Health Care System.<br/><br/>For example, physicians are using beta-blockers to treat <a href="https://my.clevelandclinic.org/health/diseases/16560-postural-orthostatic-tachycardia-syndrome-pots">postural tachycardia syndrome (POTS)</a>, a symptom of long COVID that happens when the heart rate increases rapidly after someone stands up or lies down. Beta-blockers, such as the off-label medication <a href="https://reference.medscape.com/drug/corlanor-ivabradine-999983">ivabradine</a>, have been used clinically to control heart rate, according to a March 2022 study published in the journal <em><a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8626157/">HeartRhythm Case Reports</a></em>.<br/><br/>“It’s not a cure, but beta-blockers can help patients manage their symptoms,” said Dr. Al-Aly.<br/><br/>Additionally, some patients respond well to low-dose <a href="https://reference.medscape.com/drug/vivitrol-revia-naltrexone-343333">naltrexone</a> for the treatment of extreme fatigue associated with long COVID. A January 2024 article in the journal <em><a href="https://pubmed.ncbi.nlm.nih.gov/38267326/">Clinical Therapeutics</a></em> found that fatigue symptoms improved in patients taking the medication.<br/><br/>Dr. Al-Aly said doctors treating patients with long COVID are getting better at pinpointing the <a href="https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8900926/">phenotype</a> or manifestation of the condition and diagnosing a treatment accordingly. Treating long COVID fatigue is not the same as treating POTS or symptoms of <a href="https://emedicine.medscape.com/article/1048596-overview">headache</a> and joint pain.<br/><br/>It’s still all about the management of symptoms and doctors lack any US Food and Drug Administration–approved medications specifically for the condition.<br/><br/></p> <h2>Clinical Trials Exploring New Therapies</h2> <p>Still, a number of large clinical trials currently underway may change that, said David F. Putrino, PhD, who runs the long COVID clinic at Mount Sinai Health System in New York City.</p> <p>Two clinical trials headed by <a href="https://www.mountsinai.org/about/newsroom/2024/mount-sinai-receives-26-million-grant-from-polybio-research-foundation-for-long-covid-clinical-trials%2523:~:text=This%252520study%252520will%252520test%252520whether,result%252520of%252520the%252520antiviral%252520treatment.">Dr. Putrino’s lab</a> are looking into repurposing two HIV antivirals to see whether they affect the levels of circulating SARS-CoV-2 virus in the body that may cause long COVID. The hope is that the antivirals Truvada and <a href="https://reference.medscape.com/drug/selzentry-maraviroc-342638">maraviroc</a> can reduce the «reactivation of latent virus» that, said Dr. Putrino, causes lingering long COVID symptoms.<br/><br/>Ongoing trials are looking into the promise of <a href="https://classic.clinicaltrials.gov/ct2/show/NCT05877508">SARS-CoV-2 monoclonal antibodies</a>, produced from cells made by cloning a unique white blood cell, as a treatment option. The trials are investigating whether these antibodies may similarly target viral reservoirs that are causing persistence of symptoms in some patients.<br/><br/>Other trials are underway through the National Institutes of Health (NIH) RECOVER initiative in which more than 17,000 patients are enrolled, the largest study of its kind, said Grace McComsey, MD.<br/><br/>Dr. McComsey, who leads the study at University Hospitals Health System in Cleveland, said that after following patients for up to 4 years researchers have gathered “a massive repository of information” they hope will help scientists crack the code of this very complex disease.<br/><br/>She and other RECOVER researchers have recently published studies on a variety of findings, reporting in February, for example, that COVID infections may <a href="https://www.researchgate.net/publication/378126313_New-onset_autoimmune_disease_after_COVID-19">trigger other autoimmune diseases</a> such as <a href="https://emedicine.medscape.com/article/331715-overview">rheumatoid arthritis</a> and <a href="https://emedicine.medscape.com/article/117853-overview">type 2 diabetes</a>. Another recent finding showed that <a href="https://www.researchgate.net/profile/Grace-Mccomsey">people with HIV</a> are at a higher risk for complications due to acute COVID-19.<br/><br/></p> <h2>Lack of Urgency Holds Back Progress</h2> <p>Still, others like Dr. Al-Aly and Dr. Putrino felt that the initiative isn’t moving fast enough. Dr. Al-Aly said that the NIH needs to “get its act together” and do more for long COVID. In the future, he said that we need to double down on our efforts to expand funding and increase urgency to better understand the mechanism of disease, risk factors, and treatments, as well as societal and economic implications.</p> <p>“We did trials for COVID-19 vaccines at warp speed, but we’re doing trials for long COVID at a snail’s pace,” he said.<br/><br/>Dr. Al-Aly is concerned about the chronic nature of the disease and how it affects patients down the line. His large-scale study published last month in the journal <em><a href="https://www.science.org/doi/10.1126/science.adl0867">Science</a></em> looked specifically at <a href="https://emedicine.medscape.com/article/235980-overview">chronic fatigue syndrome</a> triggered by the infection and its long-term impact on patients.<br/><br/>He’s concerned about the practical implications for people who are weighted down with symptoms for multiple years.<br/><br/>“Being fatigued and ill for a few months is one thing, but being at home for 5 years is a totally different ballgame.”<span class="end"/></p> <p> <em>A version of this article first appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/years-sobering-look-long-covid-progress-2024a10007a8">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>
Recently Immunized Febrile Infants Have Low Infection Risk
TOPLINE:
METHODOLOGY:
- Researchers evaluated 508 infants aged 6-12 weeks who presented with a fever of 38 °C or greater at two US military academic emergency departments (EDs) over a span of 4 years.
- The infants were categorized as “recently immunized” if they had received immunizations within 72 hours before ED presentation and “not recently immunized” if they had not. Among the 508 infants, 114 were immunized recently.
- The primary outcome was the prevalence of a serious bacterial infection (SBI), categorized into IBI and non-IBI on the basis of culture and radiography findings.
TAKEAWAY:
- The prevalence of SBI was 3.5% in the recently immunized febrile infants and 13.7% in not recently immunized febrile infants.
- Among the recently immunized infants, the prevalence of SBI was lower in those immunized within the first 24 hours than those immunized more than 24 hours before ED presentation (2% vs 14.3%, respectively).
- Almost all identified SBI cases were of urinary tract infection (UTI), with the only non-UTI case being pneumonia in an infant who exhibited respiratory symptoms within 24 hours of receiving immunization.
IN PRACTICE:
Physicians should discuss the possibilities of a less invasive approach for evaluating recently immunized febrile infants. The study findings support the general recommendation to obtain a urinalysis for all recently immunized infants over 60 days presenting with fever, including those presenting less than 24 hours post immunization.
SOURCE:
This study, led by Kyla Casey, MD, Department of Emergency Medicine, Naval Medical Center San Diego, was published online in The American Journal of Emergency Medicine.
LIMITATIONS:
The small sample size and retrospective design might have resulted in an overestimation of outcomes like IBIs within 24 hours after immunization. As the study was conducted in a specific clinical setting with febrile infants from military medical centers, the findings may have limited generalizability. Moreover, the inclusion of premature infants without age correction for prematurity could have impacted the prevalence of IBIs. Factors like missing vaccination history, healthcare referral patterns, and immunization practices in the military system may have introduced bias.
DISCLOSURE:
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors. The authors had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers evaluated 508 infants aged 6-12 weeks who presented with a fever of 38 °C or greater at two US military academic emergency departments (EDs) over a span of 4 years.
- The infants were categorized as “recently immunized” if they had received immunizations within 72 hours before ED presentation and “not recently immunized” if they had not. Among the 508 infants, 114 were immunized recently.
- The primary outcome was the prevalence of a serious bacterial infection (SBI), categorized into IBI and non-IBI on the basis of culture and radiography findings.
TAKEAWAY:
- The prevalence of SBI was 3.5% in the recently immunized febrile infants and 13.7% in not recently immunized febrile infants.
- Among the recently immunized infants, the prevalence of SBI was lower in those immunized within the first 24 hours than those immunized more than 24 hours before ED presentation (2% vs 14.3%, respectively).
- Almost all identified SBI cases were of urinary tract infection (UTI), with the only non-UTI case being pneumonia in an infant who exhibited respiratory symptoms within 24 hours of receiving immunization.
IN PRACTICE:
Physicians should discuss the possibilities of a less invasive approach for evaluating recently immunized febrile infants. The study findings support the general recommendation to obtain a urinalysis for all recently immunized infants over 60 days presenting with fever, including those presenting less than 24 hours post immunization.
SOURCE:
This study, led by Kyla Casey, MD, Department of Emergency Medicine, Naval Medical Center San Diego, was published online in The American Journal of Emergency Medicine.
LIMITATIONS:
The small sample size and retrospective design might have resulted in an overestimation of outcomes like IBIs within 24 hours after immunization. As the study was conducted in a specific clinical setting with febrile infants from military medical centers, the findings may have limited generalizability. Moreover, the inclusion of premature infants without age correction for prematurity could have impacted the prevalence of IBIs. Factors like missing vaccination history, healthcare referral patterns, and immunization practices in the military system may have introduced bias.
DISCLOSURE:
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors. The authors had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Researchers evaluated 508 infants aged 6-12 weeks who presented with a fever of 38 °C or greater at two US military academic emergency departments (EDs) over a span of 4 years.
- The infants were categorized as “recently immunized” if they had received immunizations within 72 hours before ED presentation and “not recently immunized” if they had not. Among the 508 infants, 114 were immunized recently.
- The primary outcome was the prevalence of a serious bacterial infection (SBI), categorized into IBI and non-IBI on the basis of culture and radiography findings.
TAKEAWAY:
- The prevalence of SBI was 3.5% in the recently immunized febrile infants and 13.7% in not recently immunized febrile infants.
- Among the recently immunized infants, the prevalence of SBI was lower in those immunized within the first 24 hours than those immunized more than 24 hours before ED presentation (2% vs 14.3%, respectively).
- Almost all identified SBI cases were of urinary tract infection (UTI), with the only non-UTI case being pneumonia in an infant who exhibited respiratory symptoms within 24 hours of receiving immunization.
IN PRACTICE:
Physicians should discuss the possibilities of a less invasive approach for evaluating recently immunized febrile infants. The study findings support the general recommendation to obtain a urinalysis for all recently immunized infants over 60 days presenting with fever, including those presenting less than 24 hours post immunization.
SOURCE:
This study, led by Kyla Casey, MD, Department of Emergency Medicine, Naval Medical Center San Diego, was published online in The American Journal of Emergency Medicine.
LIMITATIONS:
The small sample size and retrospective design might have resulted in an overestimation of outcomes like IBIs within 24 hours after immunization. As the study was conducted in a specific clinical setting with febrile infants from military medical centers, the findings may have limited generalizability. Moreover, the inclusion of premature infants without age correction for prematurity could have impacted the prevalence of IBIs. Factors like missing vaccination history, healthcare referral patterns, and immunization practices in the military system may have introduced bias.
DISCLOSURE:
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors. The authors had no conflicts of interest to disclose.
A version of this article appeared on Medscape.com.
<!--$RCSfile: InCopy_agile.xsl,v $ $Revision: 1.35 $-->
<!--$RCSfile: drupal.xsl,v $ $Revision: 1.7 $-->
<root generator="drupal.xsl" gversion="1.7"> <header> <fileName>167736</fileName> <TBEID>0C04F9E6.SIG</TBEID> <TBUniqueIdentifier>MD_0C04F9E6</TBUniqueIdentifier> <newsOrJournal>News</newsOrJournal> <publisherName>Frontline Medical Communications</publisherName> <storyname>recently immunized febrile infan</storyname> <articleType>2</articleType> <TBLocation>QC Done-All Pubs</TBLocation> <QCDate>20240417T093845</QCDate> <firstPublished>20240417T100059</firstPublished> <LastPublished>20240417T100059</LastPublished> <pubStatus qcode="stat:"/> <embargoDate/> <killDate/> <CMSDate>20240417T100058</CMSDate> <articleSource/> <facebookInfo/> <meetingNumber/> <byline>Zeel Mehta</byline> <bylineText>ZEEL MEHTA</bylineText> <bylineFull>ZEEL MEHTA</bylineFull> <bylineTitleText/> <USOrGlobal/> <wireDocType/> <newsDocType>News</newsDocType> <journalDocType/> <linkLabel/> <pageRange/> <citation/> <quizID/> <indexIssueDate/> <itemClass qcode="ninat:text"/> <provider qcode="provider:imng"> <name>IMNG Medical Media</name> <rightsInfo> <copyrightHolder> <name>Frontline Medical News</name> </copyrightHolder> <copyrightNotice>Copyright (c) 2015 Frontline Medical News, a Frontline Medical Communications Inc. company. All rights reserved. This material may not be published, broadcast, copied, or otherwise reproduced or distributed without the prior written permission of Frontline Medical Communications Inc.</copyrightNotice> </rightsInfo> </provider> <abstract/> <metaDescription>Recently immunized febrile infants aged 6-12 weeks exhibited a low risk for invasive bacterial infections (IBIs), with a significantly lower risk for non-IBI wi</metaDescription> <articlePDF/> <teaserImage/> <teaser>The study findings support the general recommendation to obtain a urinalysis for all recently immunized infants over 60 days presenting with fever.</teaser> <title>Recently Immunized Febrile Infants Have Low Infection Risk</title> <deck/> <disclaimer/> <AuthorList/> <articleURL/> <doi/> <pubMedID/> <publishXMLStatus/> <publishXMLVersion>1</publishXMLVersion> <useEISSN>0</useEISSN> <urgency/> <pubPubdateYear>2024</pubPubdateYear> <pubPubdateMonth/> <pubPubdateDay/> <pubVolume/> <pubNumber/> <wireChannels/> <primaryCMSID/> <CMSIDs/> <keywords/> <seeAlsos/> <publications_g> <publicationData> <publicationCode>FP</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> <journalTitle/> <journalFullTitle/> <copyrightStatement>Copyright 2017 Frontline Medical News</copyrightStatement> </publicationData> <publicationData> <publicationCode>IDPrac</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> <journalTitle/> <journalFullTitle/> <copyrightStatement/> </publicationData> <publicationData> <publicationCode>PN</publicationCode> <pubIssueName/> <pubArticleType/> <pubTopics/> <pubCategories/> <pubSections/> <journalTitle/> <journalFullTitle/> <copyrightStatement/> </publicationData> </publications_g> <publications> <term>15</term> <term>20</term> <term canonical="true">25</term> </publications> <sections> <term canonical="true">27970</term> <term>39313</term> </sections> <topics> <term>311</term> <term canonical="true">234</term> <term>271</term> </topics> <links/> </header> <itemSet> <newsItem> <itemMeta> <itemRole>Main</itemRole> <itemClass>text</itemClass> <title>Recently Immunized Febrile Infants Have Low Infection Risk</title> <deck/> </itemMeta> <itemContent> <h2>TOPLINE:</h2> <p> <span class="tag metaDescription">Recently immunized febrile infants aged 6-12 weeks exhibited a low risk for invasive bacterial infections (IBIs), with a significantly lower risk for non-IBI within the first 24 hours after immunization versus nonrecently immunized infants.</span> </p> <h2>METHODOLOGY:</h2> <ul class="body"> <li>Researchers evaluated 508 infants aged 6-12 weeks who presented with a fever of 38 °C or greater at two US military academic emergency departments (EDs) over a span of 4 years.</li> <li>The infants were categorized as “recently immunized” if they had received immunizations within 72 hours before ED presentation and “not recently immunized” if they had not. Among the 508 infants, 114 were immunized recently.</li> <li>The primary outcome was the prevalence of a serious bacterial infection (SBI), categorized into IBI and non-IBI on the basis of culture and radiography findings.</li> </ul> <h2>TAKEAWAY:</h2> <ul class="body"> <li>The prevalence of SBI was 3.5% in the recently immunized febrile infants and 13.7% in not recently immunized febrile infants.</li> <li>Among the recently immunized infants, the prevalence of SBI was lower in those immunized within the first 24 hours than those immunized more than 24 hours before ED presentation (2% vs 14.3%, respectively).</li> <li>Almost all identified SBI cases were of urinary tract infection (UTI), with the only non-UTI case being pneumonia in an infant who exhibited respiratory symptoms within 24 hours of receiving immunization.</li> </ul> <h2>IN PRACTICE:</h2> <p>Physicians should discuss the possibilities of a less invasive approach for evaluating recently immunized febrile infants. The study findings support the general recommendation to obtain a urinalysis for all recently immunized infants over 60 days presenting with fever, including those presenting less than 24 hours post immunization.</p> <h2>SOURCE:</h2> <p>This study, led by Kyla Casey, MD, Department of Emergency Medicine, Naval Medical Center San Diego, was <a href="https://doi.org/10.1016/j.ajem.2024.03.025">published online</a> in <em>The American Journal of Emergency Medicine</em>.</p> <h2>LIMITATIONS:</h2> <p>The small sample size and retrospective design might have resulted in an overestimation of outcomes like IBIs within 24 hours after immunization. As the study was conducted in a specific clinical setting with febrile infants from military medical centers, the findings may have limited generalizability. Moreover, the inclusion of premature infants without age correction for prematurity could have impacted the prevalence of IBIs. Factors like missing vaccination history, healthcare referral patterns, and immunization practices in the military system may have introduced bias.</p> <h2>DISCLOSURE:</h2> <p>This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors. The authors had no conflicts of interest to disclose.</p> <p> <em>A version of this article appeared on <span class="Hyperlink"><a href="https://www.medscape.com/viewarticle/recently-immunized-febrile-infants-have-low-infection-risk-2024a100073y">Medscape.com</a></span>.</em> </p> </itemContent> </newsItem> <newsItem> <itemMeta> <itemRole>teaser</itemRole> <itemClass>text</itemClass> <title/> <deck/> </itemMeta> <itemContent> </itemContent> </newsItem> </itemSet></root>